

Safety and efficacy of glofitamab for relapsed/refractory large B-cell lymphoma in a multinational real-world study
- PMID: 39661985
- PMCID: PMC12332916
- DOI: 10.1182/bloodadvances.2024014903
Safety and efficacy of glofitamab for relapsed/refractory large B-cell lymphoma in a multinational real-world study
Abstract
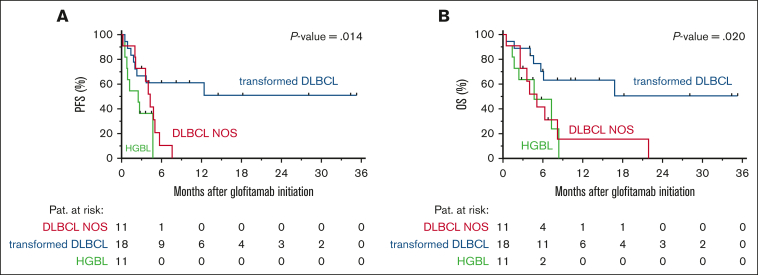
Glofitamab, a bispecific antibody targeting CD20 and CD3, is approved for relapsed/refractory diffuse large B-cell lymphoma (r/r DLBCL) after at least 2 prior treatment lines, but real-world data are scarce. In this retrospective, multicenter, multinational study, we evaluated the outcomes of 70 patients with r/r DLBCL treated with glofitamab as part of the compassionate use patient program in Germany, Austria, and Switzerland. The median number of prior treatment lines was 4, with 71% of patients refractory to their last treatment. Cytokine release syndrome was observed in 40% of patients (grade 3-4 in 2%), immune effector cell-associated neurotoxicity syndrome in 10% (grade 3 in 1%), and infections in 31% (grade 5 in 3%). The overall response rate was 46%, with 27% achieving complete responses (CR) and 19% partial responses. The median progression-free survival (PFS) was 3.6 months, whereas the median overall survival was 5.7 months. Notably, 13 patients (19%) were in CR 6 months after initiating glofitamab and exhibited durable responses. Elevated lactate dehydrogenase is the most robust predictor of inferior outcome. Patients pretreated with bendamustine within 6 months prior to glofitamab initiation exhibited significantly reduced PFS, suggesting that bendamustine may impair T-cell fitness and hence glofitamab efficacy. In summary, glofitamab demonstrates promising efficacy and a manageable safety profile in heavily pretreated patients with r/r DLBCL in a real-world scenario and the optimal sequence of treatments should use T-cell-depleting agents before glofitamab with caution.
© 2025 American Society of Hematology. Published by Elsevier Inc. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: B.C. is an inventor on patent applications related to molecular subtyping of diffuse large B-cell lymphoma, including DLB
Figures




References
-
- Swerdlow SH, Campo E, Harris NL, et al. 5th ed. International Agency for Research on Cancer; 2008. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues.
-
- Locke FL, Miklos DB, Jacobson CA, et al. Axicabtagene ciloleucel as second-line therapy for large B-cell lymphoma. N Engl J Med. 2022;386(7):640–654. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
