

Therapeutic interventions targeting enteropathy in severe acute malnutrition modulate systemic and vascular inflammation and epithelial regeneration
- PMID: 39662176
- PMCID: PMC11697704
- DOI: 10.1016/j.ebiom.2024.105478
Therapeutic interventions targeting enteropathy in severe acute malnutrition modulate systemic and vascular inflammation and epithelial regeneration
Abstract
Background: Severe acute malnutrition (SAM) is the most life-threatening form of undernutrition, and children hospitalised with complications have unacceptably high mortality. Complicated SAM is a multisystem disease characterised pathophysiologically by muscle wasting, systemic inflammation, metabolic dysfunction, and malnutrition enteropathy including epithelial barrier dysfunction. There is a clear need for novel interventions to address the underlying pathogenic perturbations of complicated SAM.
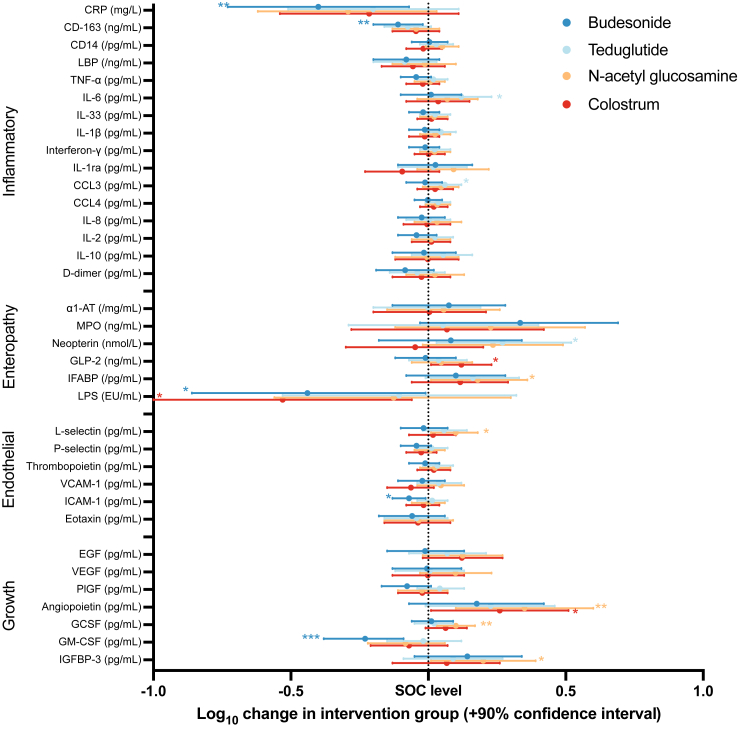
Methods: In this analysis of tertiary outcomes from a phase II multi-centre trial in Zambia and Zimbabwe, multiplex biomarkers were measured in 122 children (57% male) with SAM randomised following stabilisation ('baseline') to one of four interventions for 14 days to treat malnutrition enteropathy: budesonide, N-acetylglucosamine, colostrum, or teduglutide, compared with standard-of-care. Following measurement of 35 biomarkers from day 15 plasma samples using Luminex and ELISA, the dimensionality of biomarker data was reduced using principal component analysis.
Findings: Both budesonide and colostrum reduced systemic inflammation (as measured by CD14, IL1-ra, CRP, and LBP), while children receiving colostrum had higher GLP2 and angiopoietin, and lower circulating lipopolysaccharide, suggesting better restoration of epithelial barrier function. N-acetylglucosamine, a precursor for epithelial glycosaminoglycan synthesis, increased biomarkers of epithelial regeneration (EGF, VEGF), and circulating growth factors (angiopoietin, IGFBP-3, and GCSF).
Interpretation: Interventions aimed at ameliorating malnutrition enteropathy showed plausible effects on biomarkers of inflammation and epithelial regeneration, demonstrating an interdependence of systemic inflammation and enteropathy markers seen in structural analysis. Given the interplay between inflammation and tissue restoration in malnutrition, this mechanism of action supports larger trials to determine the clinical benefits of interventions, either alone or in combination, in children with complicated SAM.
Funding: This analysis of tertiary outcomes for the TAME trial was funded by a Wellcome grant to JPS (220566/Z/20/Z). The TAME trial was funded by a grant from the Medical Research Council (UK), number MR/P024033/1. AJP is funded by Wellcome (108065/Z/15/Z). Takeda UK provided teduglutide at a discounted price.
Keywords: Randomised trial; SAM; Severe acute malnutrition; Severe malnutrition; Systemic inflammation; Vascular inflammation.
Copyright © 2024 The Author(s). Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests RJP was previously an external consultant to Colostrum UK which provided the bovine colostrum used in these studies. RJP has also been an external consultant to Sterling Technology (USA) and an employee of Pantheryx Inc (USA) who produce and distribute bovine colostrum. There was no bovine colostrum company involvement in the production of this article or editing of its content. SH has had funding for teduglutide studies and lectured and participated in advisory boards on behalf of Takeda.
Figures



References
-
- World Health Organization . World Health Organization; 2023. Levels and Trends in Child Malnutrition: UNICEF/WHO/World Bank Group Joint Child Malnutrition Estimates: Key Findings of the 2023 Edition.
-
- World Health Organization . World Health Organization; 2013. Guideline: Updates on the Management of Severe Acute Malnutrition in Infants and Children. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
