

IL-33 is associated with alveolar dysfunction in patients with viral lower respiratory tract disease
- PMID: 39662674
- PMCID: PMC11982439
- DOI: 10.1016/j.mucimm.2024.12.001
IL-33 is associated with alveolar dysfunction in patients with viral lower respiratory tract disease
Abstract
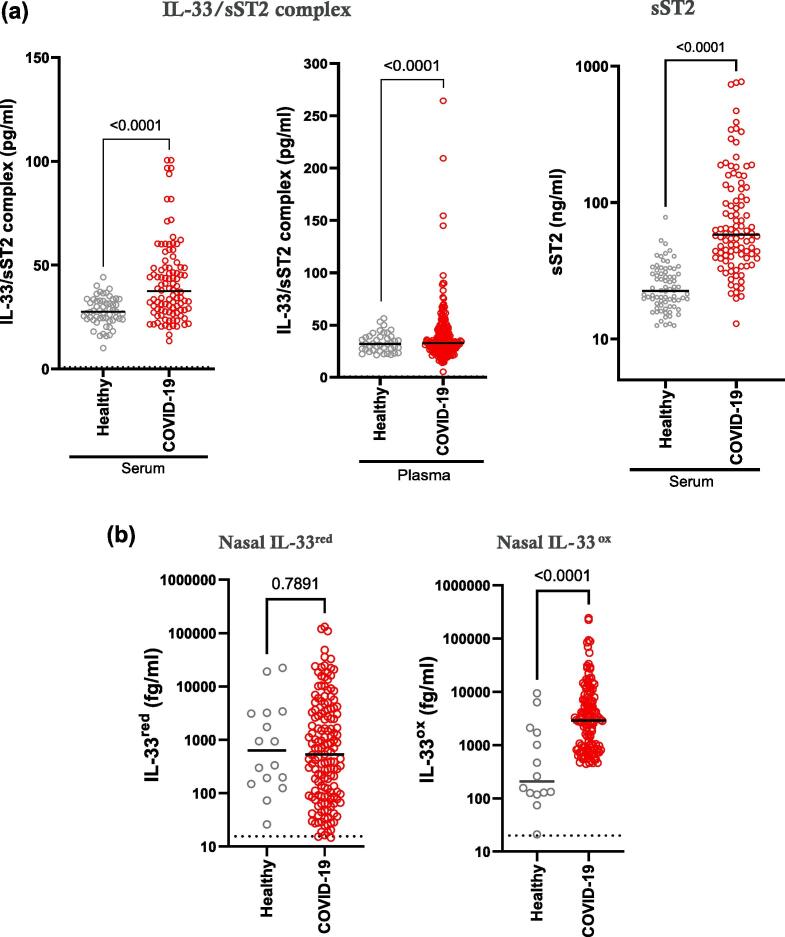
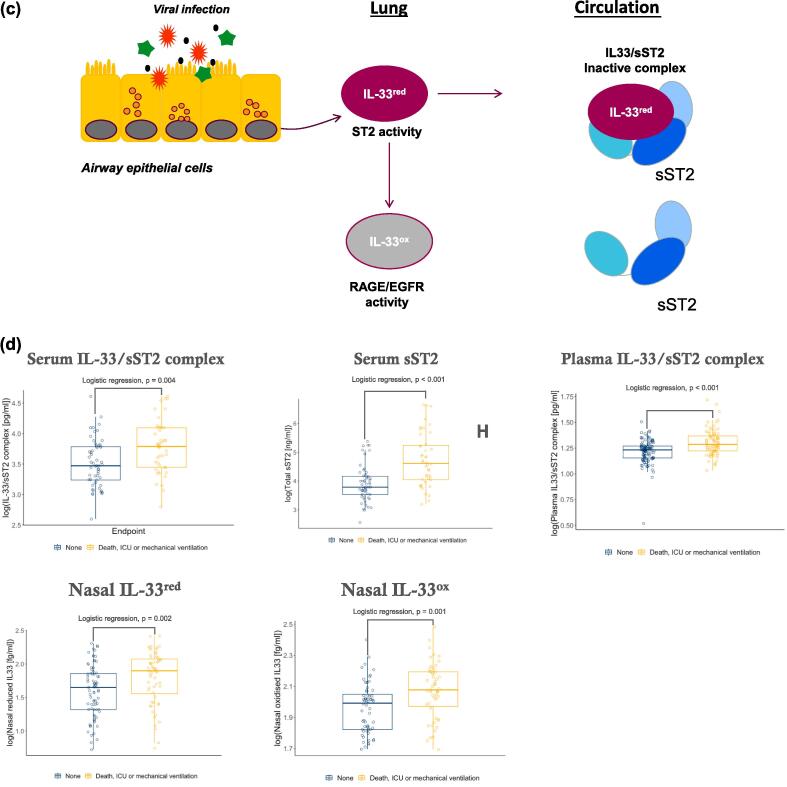
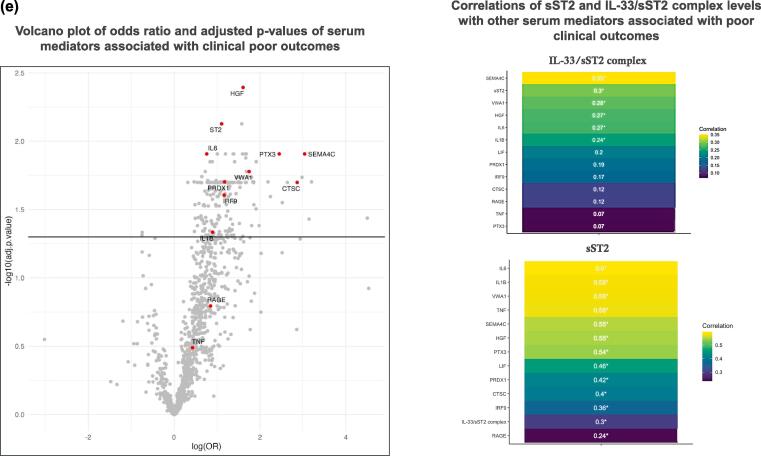
Interleukin (IL)-33 is released following tissue damage, causing airway inflammation and remodelling via reduced IL-33 (IL-33red)/serum stimulation-2 (ST2) and oxidised IL-33 (IL-33ox)/receptor for advanced glycation end products (RAGE)/epidermal growth factor receptor (EGFR) pathways. This study aimed to identify associations of IL-33 with clinical outcomes and pathological mechanisms during viral lower respiratory tract disease (LRTD). Ultra-sensitive immunoassays were developed to measure IL-33red, IL-33ox and IL-33/sST2 complexes in samples from patients hospitalised with COVID-19. Immunohistochemistry and multiomics were used to characterise lung samples. Elevated IL-33 in the airway and IL-33/sST2 complex in the circulation correlated with poor clinical outcomes (death, need for intensive care or mechanical ventilation). IL-33 was localised to airway epithelial and endothelial barriers, whereas IL1RL1 was expressed on aerocytes, alveolar endothelial cells specialised for gaseous exchange. IL-33 increased expression of mediators of neutrophilic inflammation, immune cell infiltration, interferon signalling and coagulation in endothelial cell cultures. Endothelial IL-33 signatures were strongly related with signatures associated with viral LRTD. Increased IL-33 release following respiratory viral infections is associated with poor clinical outcomes and might contribute to alveolar dysfunction. Although this does not show a causal relationship with disease, these results provide a rationale to evaluate pathological roles for IL-33 in viral LRTD.
Keywords: Aerocyte; Alarmin; Alveolar; COVID-19; IL-33; Viral LRTD.
Copyright © 2025 AstraZeneca UK LTD. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declarations of competing interests ICS, NVZ, VAN, KT, HK, ZL, CM, DGR, EE, MG, KH, ESC, ZB, DS, AF and AP are employees of AstraZeneca and may hold stock or stock options in AstraZeneca. JAC is a former employee of AstraZeneca and may hold stock or stock options in AstraZeneca. PJMO has received fees for scientific advisory boards from GSK, Moderna, Seqirus, Janssen and Sanofi Pasteur. MGS has received grants from the Department of Health and Social Care National Institute for Heath and Care Research, MRC, HPRU in Emerging and Zoonotic Infections, and the University of Liverpool during the conduct of the study; and has received other grants from Integrum Scientific LLC and Greensboro outside the submitted work. TW has received grants and fees from AstraZeneca, Bergenbio, Boehringer Ingelheim, Chiesi, GSK, Janssen, Olam, MMH, Synairgen, Union Chimique Belge and Valneva. DM, RT and JKB have no conflict of interests.
Figures






References
-
- Cayrol C., Girard J.P. Interleukin-33 (IL-33): A critical review of its biology and the mechanisms involved in its release as a potent extracellular cytokine. Cytokine. 2022;156 - PubMed
-
- Rabe K.F., Celli B.R., Wechsler M.E., et al. Safety and efficacy of itepekimab in patients with moderate-to-severe COPD: a genetic association study and randomised, double-blind, phase 2a trial. Lancet Respir Med. 2021;9:1288–1298. - PubMed
-
- Wechsler M.E., Ruddy M.K., Pavord I.D., et al. Efficacy and Safety of Itepekimab in Patients with Moderate-to-Severe Asthma. N Engl J Med. 2021;385:1656–1668. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
