

GLPp16 gene amplification induces susceptibility to high-grade urothelial carcinoma
- PMID: 39664176
- PMCID: PMC11632529
- DOI: 10.3389/fonc.2024.1495381
GLPp16 gene amplification induces susceptibility to high-grade urothelial carcinoma
Abstract
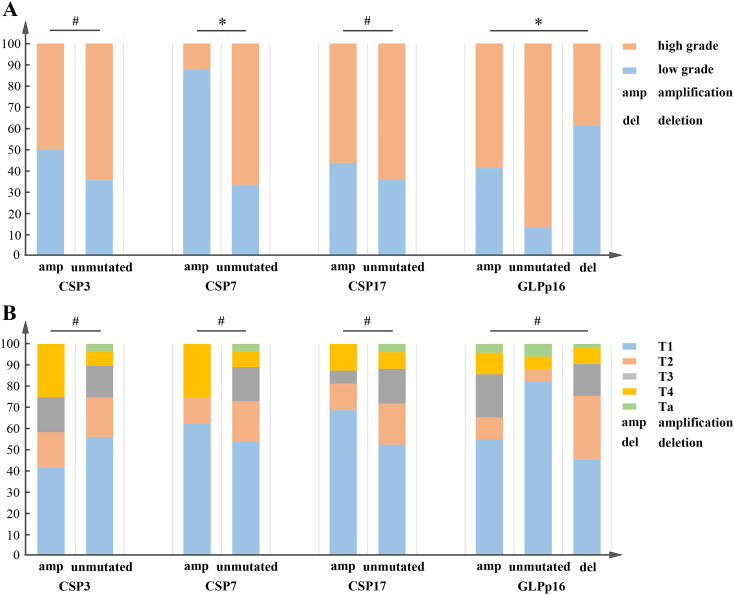
Background: Urothelial carcinoma is a common malignant tumor of the urinary system, with prognosis linked to pathological grade and TNM stage. Alterations in chromosomes 3, 7, and 17, along with the P16 locus on chromosome 9 (CSP3, CSP7, CSP17, and GLPp16), are associated with cancer progression and may serve as important biomarkers. This study aimed to explore the relationships between these chromosomal factors and the pathological grade and TNM stage of UCC, potentially leading to a novel diagnostic approach that enhances patient stratification and treatment planning.
Methods: A retrospective analysis was conducted on 149 patients to evaluate the correlation between CSP3, CSP7, CSP17, GLPp16, TNM stage, and pathological grade using chi-square tests and logistic regression. Immunohistochemistry was employed to assess the associated changes.
Results: Univariate analysis indicated that only CSP7 and GLPp16 were significantly associated with pathological grade. Logistic regression linked GLPp16 and gender to pathological grade in urothelial carcinoma. A nomogram model incorporating these factors demonstrated reliable calibration in the training set (non-significant Hosmer-Lemeshow test, P = 0.436; AUC = 0.785, 95% CI: 0.707 - 0.863) and effective discrimination in the test set (AUC = 0.740, 95% CI: 0.559 - 0.920). Immunohistochemistry revealed P16 gene deletion in low-grade urothelial carcinoma and amplification in high-grade urothelial carcinoma.
Conclusion: Mutations at the GLPp16 were significantly correlated with the pathological grade of urothelial carcinoma. Additionally, the amplification of GLPp16 was recognized as a contributing factor to the development of high-grade urothelial carcinoma.
Keywords: FISH; GLPp16; nomogram; pathological grading; urothelial carcinoma.
Copyright © 2024 Liu, Sun, Long, Zhang, Zheng and Zhang.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures




References
LinkOut - more resources
Full Text Sources