Epithelial-Mesenchymal Transition in Chronic Rhinosinusitis
- PMID: 39664411
- PMCID: PMC11566545
- DOI: 10.18787/jr.2024.00022
Epithelial-Mesenchymal Transition in Chronic Rhinosinusitis
Abstract
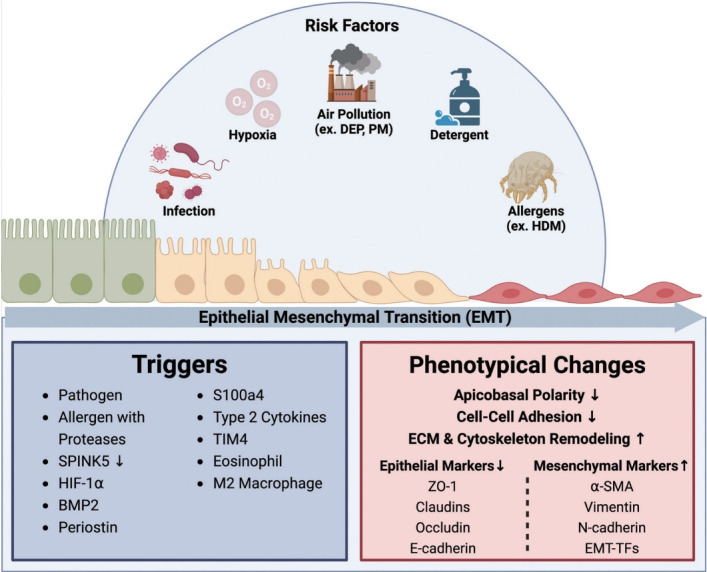
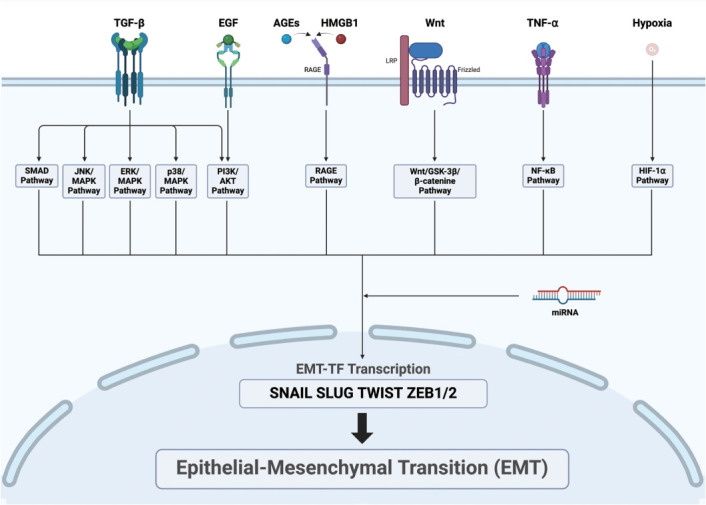
Chronic rhinosinusitis (CRS) is characterized by prolonged inflammation of the nasal and paranasal sinus mucosa lasting over 12 weeks. CRS is divided into two main types based on the presence of nasal polyps: CRS without nasal polyps and CRS with nasal polyps. The condition is further classified into endotypes based on type 1, type 2, and type 3 inflammatory signatures, with differences in terms of disease severity, prognosis, and treatment response. Recent studies have emphasized the importance of the epithelial-mesenchymal transition (EMT) in CRS progression. In CRS, the EMT can be triggered by infections, allergens, hypoxia, and environmental pollutants. Specifically, EMT induction proceeds through the following mechanisms: viral and bacterial infections disrupt the epithelial barrier, house dust mites and other allergens activate the TGF-β and EGFR signaling pathways, hypoxia increases HIF-1α and other mesenchymal markers, and diesel exhaust particles and particulate matter cause oxidative stress. Maintaining the integrity of the epithelial barrier is essential for nasal mucosa homeostasis. In CRS, barrier damage activates repair processes that trigger the EMT, resulting in barrier dysfunction and tissue remodeling. Epithelial barrier dysfunction allows antigens and pathogens to penetrate, perpetuating inflammation and promoting the EMT. This disruption is a hallmark of CRS, emphasizing the importance of barrier integrity in the development of the disease. Key signaling pathways regulating the EMT in CRS include TGF-β, Wnt, HMGB1, AGE/ERK, TNF-α, and various miRNAs. These signaling pathways connect to various downstream pathways, such as the Smad2/3, GSK-3β/β-catenin, RAGE, and NF-κB pathways. This review focuses on the complex mechanisms of the EMT in CRS, emphasizing the role of epithelial barrier dysfunction and subsequent EMT processes in driving the disease's development and progression. A deeper understanding of these EMT-driven mechanisms will help identify the potential therapeutic targets aimed at restoring epithelial integrity and reversing the EMT.
Keywords: Airway remodeling; Chronic rhinosinusitis; Epithelial-mesenchymal transition; Nasal mucosa.
Copyright © 2024 by The Korean Rhinologic Society.
Conflict of interest statement
Conflicts of Interest The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Bachert C, Marple B, Schlosser RJ, Hopkins C, Schleimer RP, Lambrecht BN, et al. Adult chronic rhinosinusitis. Nat Rev Dis Primers. 2020;6(1):86. - PubMed
-
- Sedaghat AR, Kuan EC, Scadding GK. Epidemiology of chronic rhinosinusitis: prevalence and risk factors. J Allergy Clin Immunol Pract. 2022;10(6):1395–403. - PubMed
-
- Yan B, Lan F, Li J, Wang C, Zhang L. The mucosal concept in chronic rhinosinusitis: focus on the epithelial barrier. J Allergy Clin Immunol. 2024;153(5):1206–14. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous