

Left Ventricular Reverse Remodeling after Successful Living Donor Kidney Transplantation: The Visualizing the Pathophysiology of Kidney Transplantation in Modern Age Study
- PMID: 39666313
- PMCID: PMC11970851
- DOI: 10.34067/KID.0000000673
Left Ventricular Reverse Remodeling after Successful Living Donor Kidney Transplantation: The Visualizing the Pathophysiology of Kidney Transplantation in Modern Age Study
Abstract
Key Points:
Kidney transplantation (KT) can improve even advanced left ventricular (LV) geometric patterns, but this effect may be attenuated by pre-KT decreased diastolic function and acute antibody-mediated rejection.
Regardless of the pre-KT LV geometric pattern, the postoperative LV geometric pattern tended to shift toward concentric remodeling.
Geometric patterns may be an easy-to-understand and useful cardiac function assessment tool for nephrologists.
Background: The effect of kidney transplantation (KT) on left ventricular (LV) remodeling remains poorly understood. The aim of this study was to evaluate the effect of KT on LV reverse remodeling, using echocardiographic LV geometric patterns as a key assessment tool.
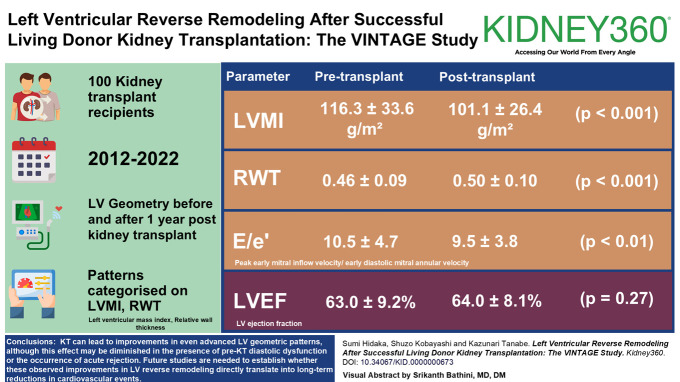
Methods: In 100 recipients who underwent living KT between 2012 and 2022, we evaluated changes in the distribution of LV geometric patterns (normal geometry, concentric remodeling [CR], eccentric hypertrophy [EH], and concentric hypertrophy [CH]) between baseline and 1 year after transplantation. These patterns were categorized on the basis of LV mass index and relative wall thickness assessed by echocardiography.
Results: Overall, LV geometric patterns improved or remained stable in 81% of recipients, with worsening in 19%. The proportion of normal geometry increased from 15% to 19% and CR from 30% to 45%, whereas EH decreased markedly from 20% to 3%. CH remained relatively stable at 33% (P = 0.036). Subgroup analysis revealed that 47% of those with pre-KT normal geometry progressed to LV remodeling, whereas 77% with CR remained stable. By contrast, 55% with EH experienced reverse remodeling and 49% with CH also showed reverse remodeling. These subgroup results suggest an interaction between the effect of KT on LV reverse remodeling and pre-KT LV geometric patterns. Multivariable analysis identified E/e′ > 9.5 (odds ratio, 2.01; 95% confidence interval, 1.10 to 3.67; P = 0.024) and acute antibody-mediated rejection (odds ratio, 2.44; 95% confidence interval, 1.01 to 5.87; P = 0.047) as independent predictors of LV remodeling progression.
Conclusions: KT can lead to improvements in even advanced LV geometric patterns, although this effect may be diminished in the presence of pre-KT diastolic dysfunction or the occurrence of acute rejection. Because recipients rarely achieve complete renal recovery, echocardiographic monitoring remains crucial after KT. Future studies are needed to establish whether these observed improvements in LV reverse remodeling directly translate into long-term reductions in cardiovascular events.
Conflict of interest statement
Disclosure forms, as provided by each author, are available with the online version of the article at
Figures





References
LinkOut - more resources
Full Text Sources
