

Evaluating generative artificial intelligence's limitations in health policy identification and interpretation
- PMID: 39666618
- PMCID: PMC11637257
- DOI: 10.1371/journal.pone.0312078
Evaluating generative artificial intelligence's limitations in health policy identification and interpretation
Abstract
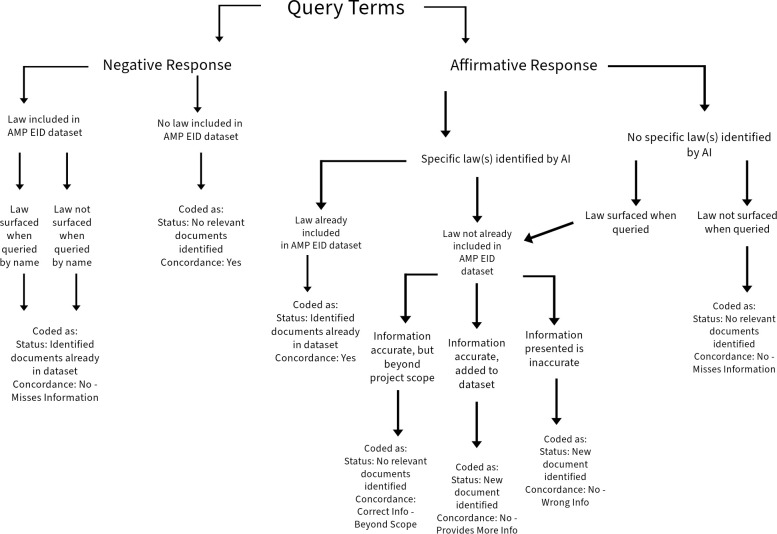
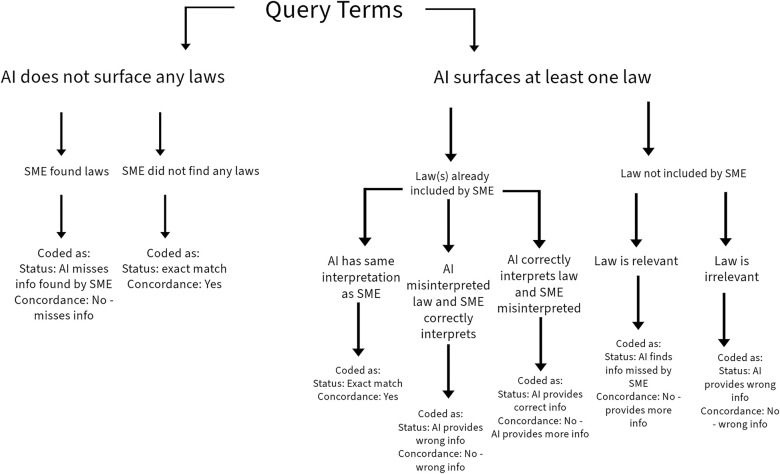
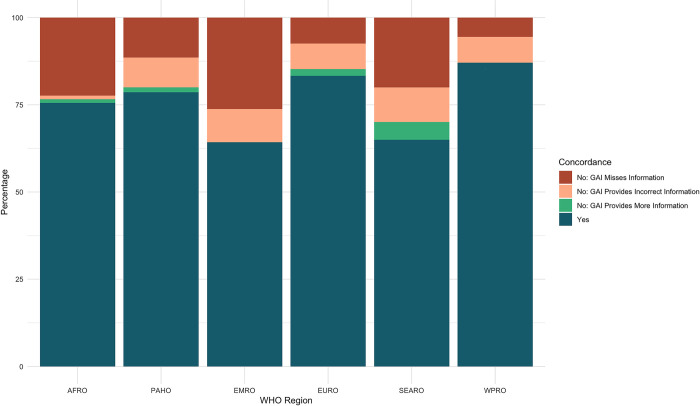
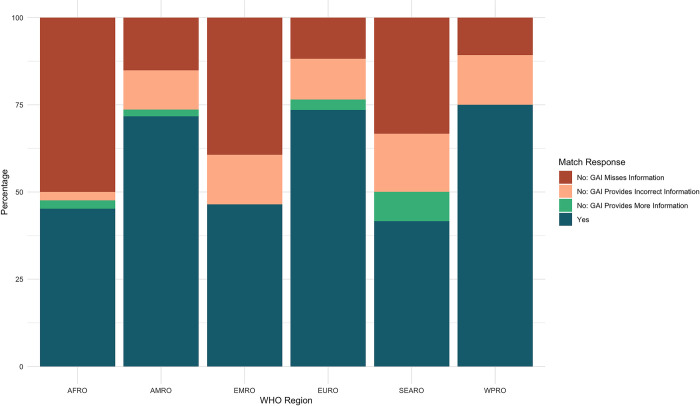
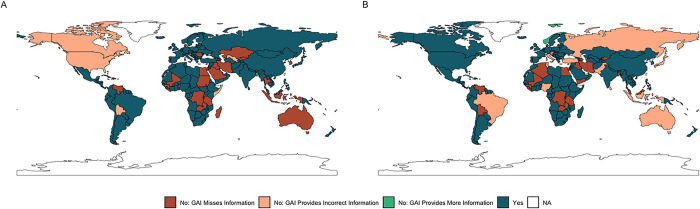
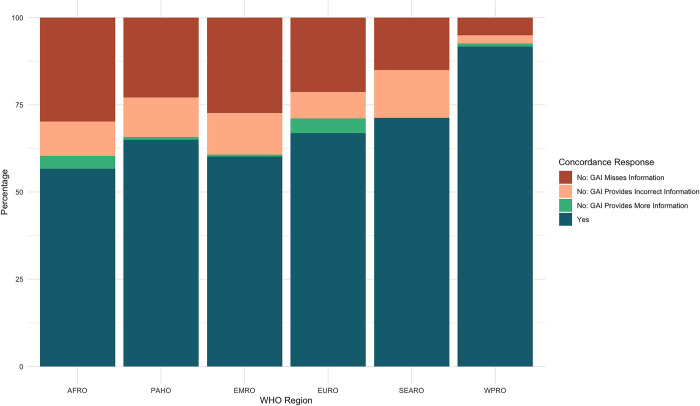
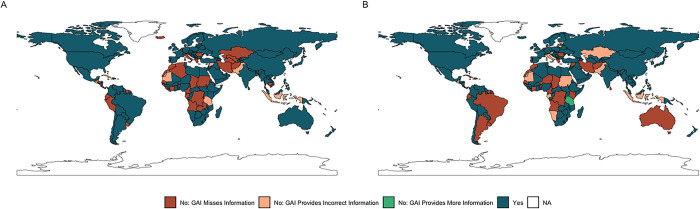
Policy epidemiology utilizes human subject-matter experts (SMEs) to systematically surface, analyze, and categorize legally-enforceable policies. The Analysis and Mapping of Policies for Emerging Infectious Diseases project systematically collects and assesses health-related policies from all United Nations Member States. The recent proliferation of generative artificial intelligence (GAI) tools powered by large language models have led to suggestions that such technologies be incorporated into our project and similar research efforts to decrease the human resources required. To test the accuracy and precision of GAI in identifying and interpreting health policies, we designed a study to systematically assess the responses produced by a GAI tool versus those produced by a SME. We used two validated policy datasets, on emergency and childhood vaccination policy and quarantine and isolation policy in each United Nations Member State. We found that the SME and GAI tool were concordant 78.09% and 67.01% of the time respectively. It also significantly hastened the data collection processes. However, our analysis of non-concordant results revealed systematic inaccuracies and imprecision across different World Health Organization regions. Regarding vaccination, over 50% of countries in the African, Southeast Asian, and Eastern Mediterranean regions were inaccurately represented in GAI responses. This trend was similar for quarantine and isolation, with the African and Eastern Mediterranean regions least concordant. Furthermore, GAI responses only provided laws or information missed by the SME 2.14% and 2.48% of the time for the vaccination dataset and for the quarantine and isolation dataset, respectively. Notably, the GAI was least concordant with the SME when tasked with policy interpretation. These results suggest that GAI tools require further development to accurately identify policies across diverse global regions and interpret context-specific information. However, we found that GAI is a useful tool for quality assurance and quality control processes in health policy identification.
Copyright: This is an open access article, free of all copyright, and may be freely reproduced, distributed, transmitted, modified, built upon, or otherwise used by anyone for any lawful purpose. The work is made available under the Creative Commons CC0 public domain dedication.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Katz R. Policy Epidemiology: Identifying What Works in Outbreak Preparedness and Response. Health Affairs. 2023. Sep 14. Available from: https://www.healthaffairs.org/content/forefront/policy-epidemiology-iden...
-
- Katz R, Graeden E, Kerr J, Eaneff S. Tracking the flow of policy: Applying a new approach for tracking the flow of health policy. Milbank Q. 2023;101(3):632–652.
-
- Ljungqvist GV, Weets CM, Stevens T, Robertson H, Zimmerman R, Graeden E, et al.. Global Patterns in Access and Benefit-Sharing: A Comprehensive Review of National Policies. medRxiv [Preprint]. 2024. Jul 12:2024.07.12.24310347.
-
- Open AI, Achiam J, Adler S, Agarwal S, Ahmad L, Akkaya I, et al.. GPT-4 Technical Report. arXiv. 2023. Mar 15:2303.08774.
MeSH terms
LinkOut - more resources
Full Text Sources
