

Flow diverter versus stent-assisted coiling treatment for managing dissecting intracranial aneurysms: A systematic review and meta-analysis
- PMID: 39668743
- PMCID: PMC11638934
- DOI: 10.1177/15910199241301820
Flow diverter versus stent-assisted coiling treatment for managing dissecting intracranial aneurysms: A systematic review and meta-analysis
Abstract
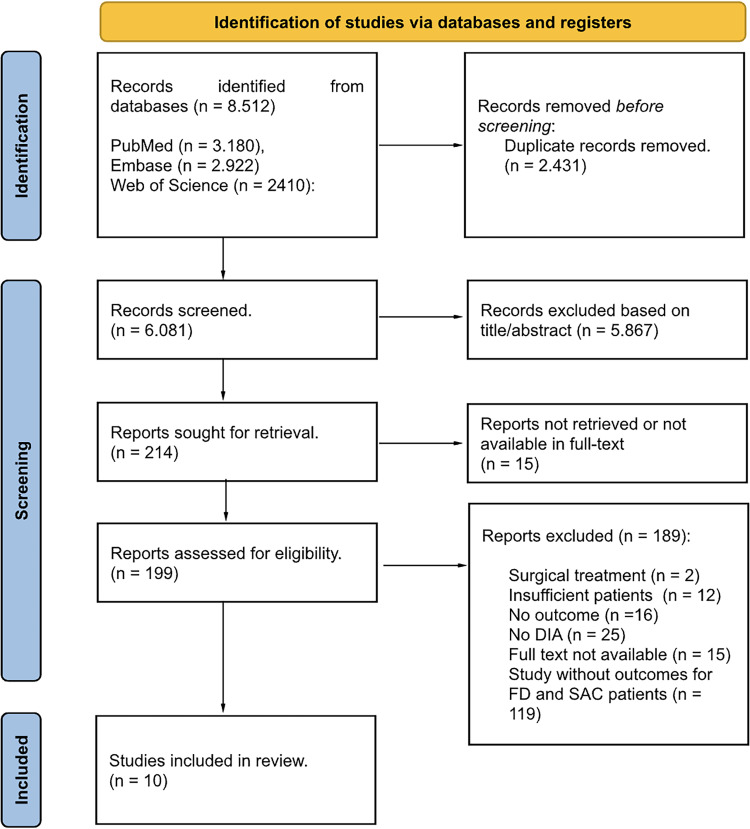
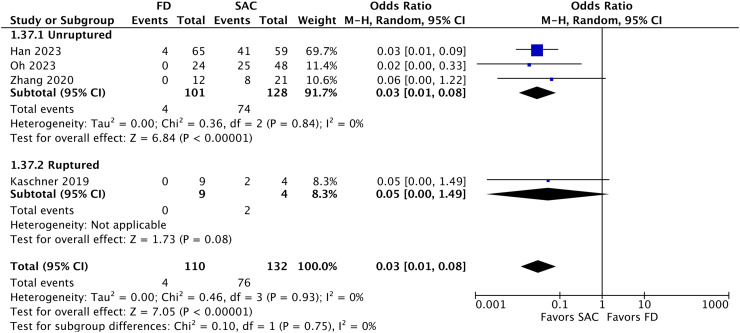
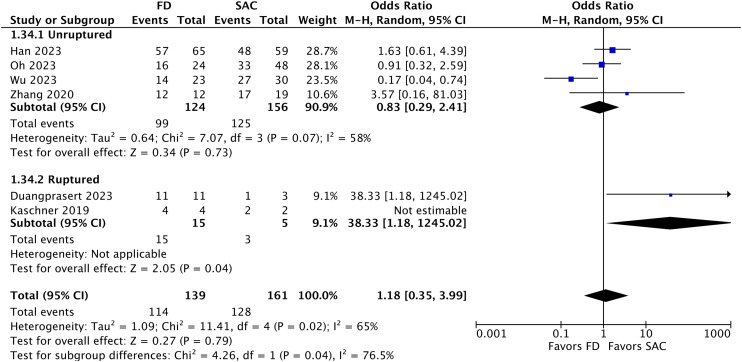
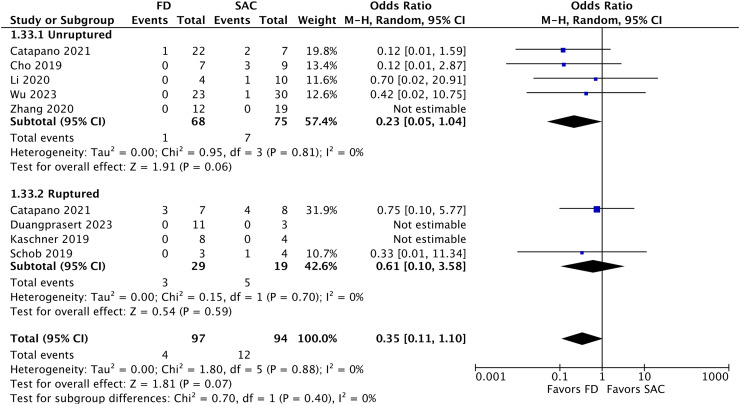
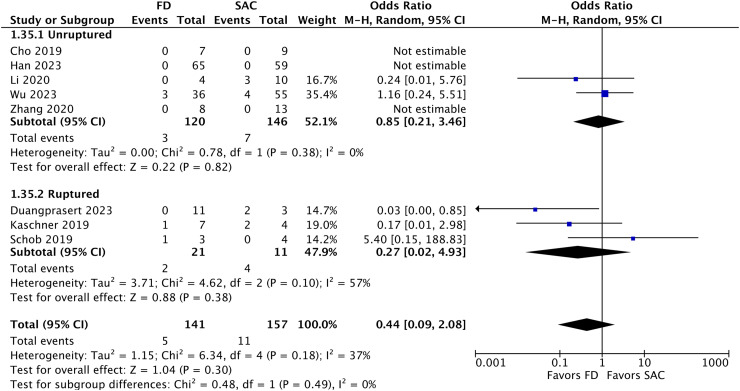
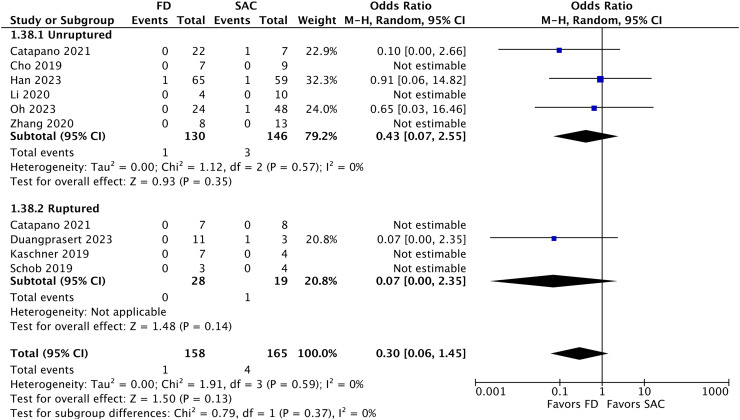
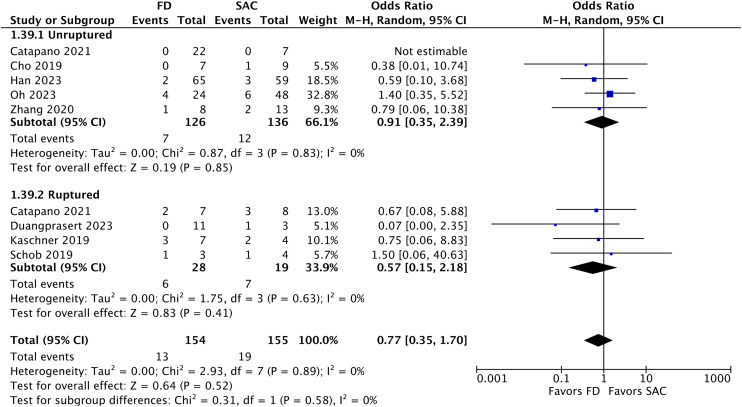
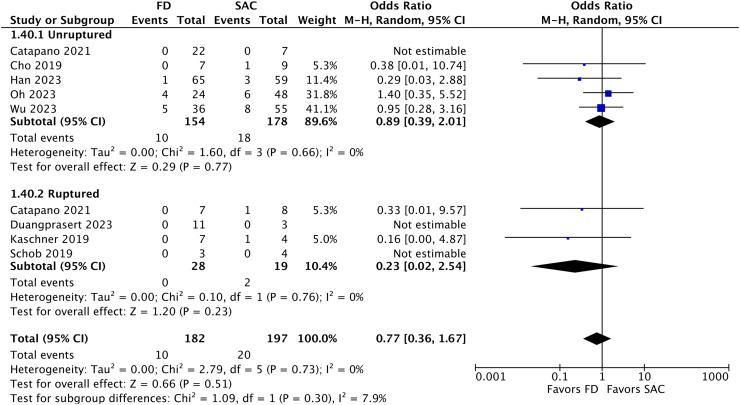
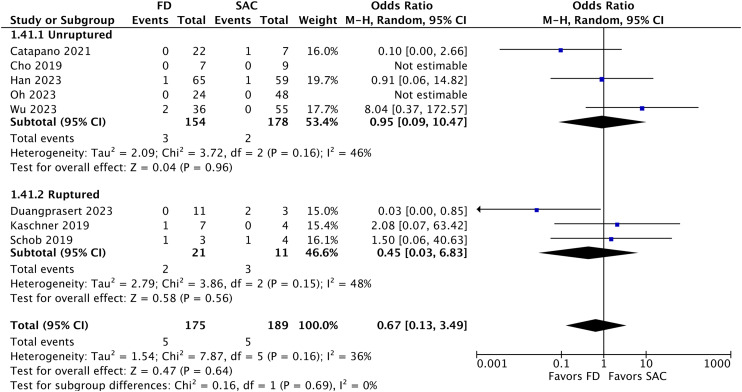
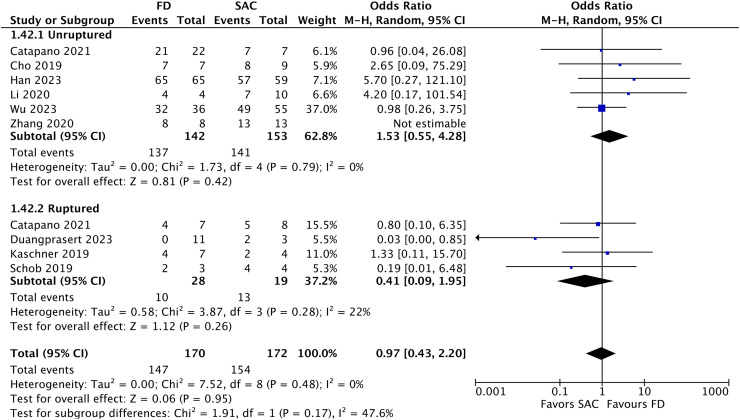
BackgroundDissecting intracranial aneurysms (DIAs) have been treated through endovascular reconstructive manners, such as flow diverters (FDs) and stent-assisted coiling (SAC). Notably, no robust evidence has compared both approaches. Hence, the authors conducted a meta-analysis to compare their outcomes.MethodsPubMed, Embase and Web of Science were searched for studies employing SAC and FD treatment for DIAs. The following outcomes were considered for extraction: procedure-related mortality, total mortality, postoperative and follow-up complete aneurysm occlusion, complications, good clinical outcomes, recurrence, and retreatment. Odds ratio (OR) with random effects was employed for statistical comparison.ResultsThe meta-analysis included 10 studies. A total of 195 and 222 patients were included in the FD and the SAC group, respectively. Stent-assisted coiling had higher postoperative complete aneurysm occlusion rates (OR 0.03; 95% CI 0.01-0.08). Flow diverter retreatment rate was lower, but without statistical significance (OR 0.35; 95% CI 0.11-1.10). No significant differences were found in follow-up complete aneurysm occlusion (OR 1.18; 95% CI 0.35-3.99); total mortality (OR 0.44; 95% CI 0.09-2.08); intraoperative complications (OR 0.30; 95% CI 0.06-1.45); postoperative complication (OR 0.77; 95% CI 0.35-1.70); good clinical outcomes (OR 0.97; 95% CI 0.43-2.20); and recurrence (OR 0.38; 95% CI 0.13-1.10) between the two groups.ConclusionStent-assisted coiling shows higher postoperative complete aneurysmal occlusion rates, but both techniques achieve similar rates in angiographic follow-up. Flow diverter has lower, but not statistically significant, retreatment rates than SAC. Both techniques have similar complication rates. Future randomized, multicenter, and prospective studies with larger sample sizes are needed for more conclusive findings.
Keywords: Stent-assisted coiling; aneurysm; coil; dissecting; flow diverter; meta-analysis; systematic review.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Bond KM, Krings T, Lanzino Get al. et al. Intracranial dissections: a pictorial review of pathophysiology, imaging features, and natural history. J Neuroradiol 2021; 48: 176–188. - PubMed
-
- Oh HS, Bae JW, Hong CE, et al. Stent-assisted coil embolization versus flow-diverting stent in unruptured vertebral artery dissecting aneurysms: efficacy and safety comparison. Neurosurgery 2023; 93: 120–127. - PubMed
-
- Liu P, Li Z, Hu L, et al. Clinical characteristics, endovascular choices, and surgical outcomes of intracranial vertebral artery dissecting aneurysms: a consecutive series of 196 patients. J Neurosurg 2022; 138: 215–222. Published June 3, 2022. - PubMed
-
- Han J, Tong X, Han M, et al. Flow diverters versus stent-assisted coiling in unruptured intracranial vertebral artery dissecting aneurysms. J Neurosurg 2024; 140: 1064–1070. Published online October 13, 2023. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
