

Clinical Outcomes of Therapeutic Interventions for Autoimmune Retinopathy: A Meta-analysis and Systematic Review
- PMID: 39669695
- PMCID: PMC11635770
- DOI: 10.1016/j.xops.2024.100622
Clinical Outcomes of Therapeutic Interventions for Autoimmune Retinopathy: A Meta-analysis and Systematic Review
Abstract
Topic: Autoimmune retinopathy (AIR) is a group of rare inflammatory diseases treated with immunosuppression; however, there is no treatment consensus. This meta-analysis and review aims to investigate treatment effectiveness in slowing AIR progression.
Clinical relevance: Autoimmune retinopathy is a group of diseases characterized by progressive vision loss that is both difficult to diagnose and treat. While there is some consensus regarding diagnostic criteria, evidence-based treatment consensus remains poorly understood. Current first-line treatment is systemic steroids and conventional steroid-sparing agents. However, patients often experience treatment failure and systemic adverse effects with these medications. Understanding the effect of medications on slowing multiple visual outcomes in AIR can help to guide future treatment protocols.
Methods: PubMed, Cochrane Library, Embase, and ClinicalTrials.gov were systematically searched from inception to November 2023. Included studies treated patients with AIR with systemic, local, and biologic therapy and reported visual acuity (VA), visual field (VF), cystoid macular edema (CME), electroretinogram, central retinal thickness (CRT), and/or ellipsoid zone (EZ) loss. Risk of bias was assessed using the Critical Appraisal Skills Programme checklist. Data for meta-analysis were pooled using a random-effects model.
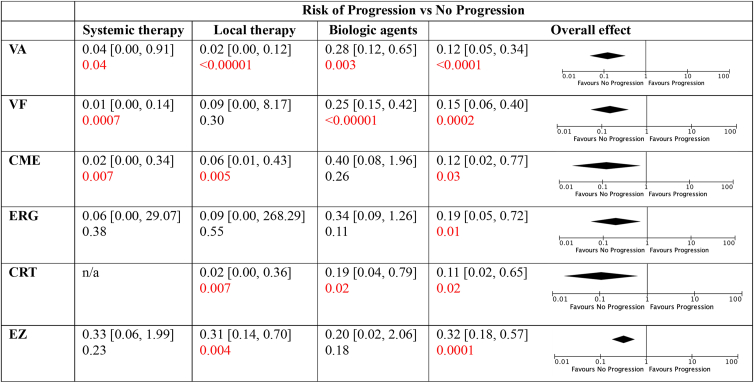
Results: Analysis of 40 case reports demonstrated that treatment type significantly affects the improvement of VA in patients with nonparaneoplastic retinopathy. Meta-analysis of 12 studies demonstrated that any treatment decreases the risk of progression of all 6 outcomes. Systemic therapy slows VA loss (risk ratio [RR] = 0.04, 95% confidence interval [0.00, 0.91], P = 0.04), VF loss (RR = 0.01, 95% confidence interval [0.00, 0.14], P = 0.0007), and CME (RR = 0.02, 95% confidence interval [0.00, 0.34], P = 0.007). Local therapy slows VA loss (RR = 0.02, 95% confidence interval [0.00, 0.12], P < 0.00001), CME (RR = 0.06, 95% confidence interval [0.01, 0.43], P = 0.005), CRT loss (RR = 0.02, 95% confidence interval [0.00, 0.36], P = 0.007), and EZ loss (RR = 0.31, 95% confidence interval [0.14, 0.70], P = 0.004). Biologics slow VA loss (RR = 0.28, 95% confidence interval [0.12, 0.65], P = 0.003), VF loss (RR = 0.25, 95% confidence interval [0.15, 0.42], P < 0.00001), and CRT loss (RR = 0.19, 95% confidence interval [0.04, 0.79], P = 0.02).
Conclusion: Systemic therapy significantly reduces the risk of progressive visual loss. Local therapy significantly decreases the risk of both progressive visual loss and retinal morphology loss, and therefore may offer precise targeting of the retina. Biologics significantly reduce both functional and morphological retinal changes. Immunosuppressive therapy may slow AIR progression; however, additional research is needed to assess long-term outcomes.
Financial disclosures: The author(s) have no proprietary or commercial interest in any materials discussed in this article.
Keywords: Autoimmune retinopathy; Biologic agents; Immunosuppression; Paraneoplastic retinopathy.
© 2024 by the American Academy of Ophthalmology.
Figures


References
-
- Sawyer R.A., Selhorst J.B., Zimmerman L.E., Hoyt W.F. Blindness caused by photoreceptor degeneration as a remote effect of cancer. Am J Ophthalmol. 1976;81:606–613. - PubMed
-
- Guy J., Aptsiauri N. Treatment of paraneoplastic visual loss with intravenous immunoglobulin: report of 3 cases. Arch Ophthalmol. 1999;117:471–477. - PubMed
-
- Comlekoglu D.U., Thompson I.A., Sen H.N. Autoimmune retinopathy. Curr Opin Ophthalmol. 2013;24:598. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
