

A feasibility model for restructuring the role of the hand surgeon taking call at a level I trauma center
- PMID: 39669723
- PMCID: PMC11632805
- DOI: 10.1016/j.jham.2024.100145
A feasibility model for restructuring the role of the hand surgeon taking call at a level I trauma center
Abstract
Background: The discrepancy between the volume of hand-related consults and the concurrent lack of specialized hand surgeons available continues to strain an overburdened system. Recent attention has focused on the redistribution of this workload towards management in the outpatient realm.
Methods: This is a retrospective review of hand consults for the plastic surgery service over summer and winter intervals at a Level I trauma center. Consults were triaged with non-plastic surgery residents managing consults through remote direction of a plastic surgery resident. Demographic, clinical and outcomes data were analyzed to make inferences regarding care.
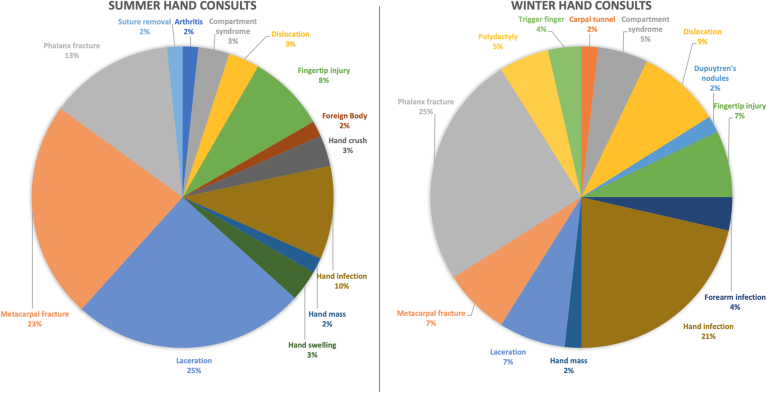
Results: There were 116 hand consults of which 94.8 % were managed acutely by non-plastic surgery clinicians. Lacerations and fractures were more common in the summer, while infections and dislocations were more common in the wintertime (p value = 0.0029). The three most common procedures were reduction and splinting (41.4 %), suturing (28.4 %), and incision and drainage (6.0 %). 12.1 % were admitted for management of the hand-related issue. Average time to the OR was shortest for infections or compartment syndrome as compared to that for other acquired concerns (1.0 days versus 11.6 days, p = 0.0027). There were two complications (1.7 %) involving an unplanned return to the OR, but neither resulted from a delay in treatment.
Conclusions: We propose a model of offloading the majority of hand consults through coverage by trainees with trauma experience knowledgeable in the basics of hand exams and general procedures. This model was safe and effective across a wide range of hand-related complaints.
Keywords: Education; Emergency department; Hand consult; Trauma; Triage.
© 2024 Society for Indian Hand Surgery and Micro Surgeons. Published by Elsevier B.V. All rights are reserved, including those for text and data mining, AI training, and similar technologies.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures

References
-
- Centers for Disease Control and Prevention. National Hospital Ambulatory Medical Care Survey: 2010 Emergency Department Summary Tables. Centers for Disease Control and Prevention. Available at: http://www.cdc.gov/nchs/data/ahcd/nhamcs_emergency/2010_ed_web_tables.pdf.
-
- Rudkin S.E., Oman J., Langdorf M.I., et al. The state of ED on-call coverage in California. Am J Emerg Med. 2004;22:575–581. - PubMed
-
- Mueller M.A., Zaydudim V., Sexton K.W., et al. Lack of emergency hand surgery: discrepancy between elective and emergency hand care. Ann Plast Surg. 2012;68:513–517. - PubMed
-
- Whipple L.A., Kelly T., Aliu O., Roth M.Z., Patel A. The crisis of deficiency in emergency coverage for hand and facial trauma: exploring the discrepancy between availability of elective and emergency surgical coverage. Ann Plast Surg. 2017;79(4):354. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous