

Evaluation of fibroinflammatory activity in thyroid eye disease using [18F]AlF-NOTA-FAPI-04 PET/CT: A prospective study
- PMID: 39671100
- PMCID: PMC11928422
- DOI: 10.1007/s00259-024-07015-y
Evaluation of fibroinflammatory activity in thyroid eye disease using [18F]AlF-NOTA-FAPI-04 PET/CT: A prospective study
Abstract
Purpose: This study evaluates the value of [18F]AlF-NOTA-FAPI-04PET/CT in assessing the disease activity of thyroid eye disease (TED).
Methods: Twenty-three TED patients and ten healthy controls were prospectively recruited and underwent [18F]AlF-NOTA-FAPI-04 PET/CT scans. TED eyes were classified by Clinical Activity Score (CAS) as active (CAS +) or inactive (CAS-). PET analysis included qualitative and quantitative evaluations. Qualitative analysis categorized TED eyes as positive (FAPI +) or negative (FAPI-), while quantitative analysis including SUVmax and target-to-backgroud ratio (TBR) of each extraocular muscle (EOM). Pathological assessment of 16 EOM samples from 15 TED eyes was used as a gold standard to evaluate the diagnostic accuracy of CAS-driven and FAPI-driven assessments.
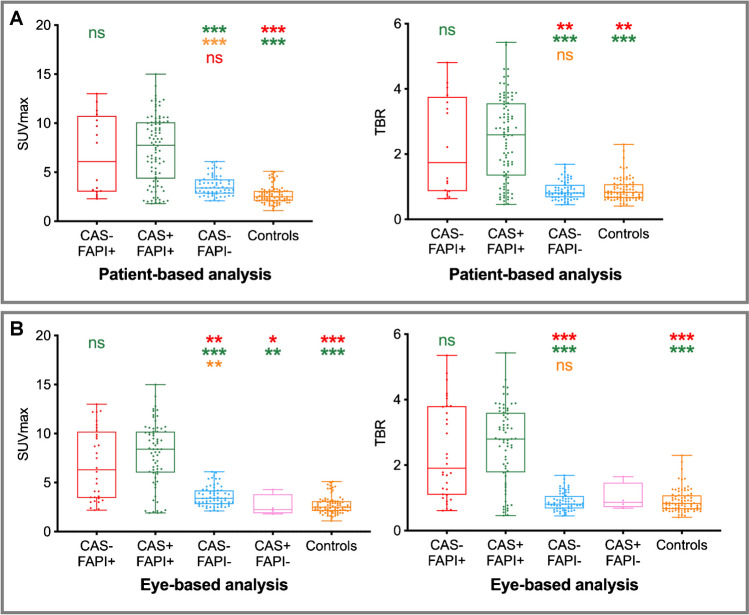
Results: Eye-based analysis included 42 TED eyes and 20 control eyes. SUVmax did not differ significantly between CAS-/FAPI + (n = 8) and CAS + /FAPI + (n = 17) eyes; though both groups had significantly higher SUVmax than CAS-/FAPI- (n = 16), CAS + /FAPI- (n = 1), and control eyes (n = 20) (all P < .05). Diffuse high FAPI uptake with excellent TBR was observed in pathologically active EOMs and had higher SUVmax and TBR than inactive EOMs (SUVmax: 9.57 ± 2.79 vs. 4.04 ± 1.02, TBR: 2.99 ± 1.00 vs. 1.00 ± 0.35, both P < .001). An SUVmax cutoff value of 5.95 yielded an area under the receiver operating characteristic curve of 0.98 for predicting active disease. Sensitivity and specificity of CAS-driven and FAPI-driven assessments for TED activity were 72.7% and 100%, 100% and 100%, respectively. SUVmax positively correlated with pathological fibroinflammatory score (r = 0.68, P = .004).
Conclusion: The diffuse high FAPI uptake with excellent TBR in the EOMs could illustrate the activity of TED, positively correlated with pathological fibroinflammatory scores. These findings suggest that [18F]AlF-NOTA-FAPI-04 PET/CT may serve as a promising reliable non-invasive approach for assessing disease activity in TED, potentially superior to the CAS.
Keywords: Clinical activity score; Extraocular muscles; Fibroblast activation protein inhibitor; Thyroid eye disease.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval: This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by the Ethics Committee of Peking University Third Hospital (M2023762 and M2024362). Consent to participate: Informed consent was obtained from all individual participants included in the study. Consent to publish: Informed consent for publication was obtained from the individual participant for whom identifying information is included in this article. Competing interests: The authors declare that they have no competing interests.
Figures




References
-
- Perros P, Neoh C, Dickinson J. Thyroid eye disease. Bmj. 2009;338: b560. 10.1136/bmj.b560. - PubMed
-
- Bartalena L, Kahaly GJ, Baldeschi L, Dayan CM, Eckstein A, Marcocci C, et al. The 2021 European Group on Graves’ orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves’ orbitopathy. Eur J Endocrinol. 2021;185:G43-g67. 10.1530/eje-21-0479. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
