

Leveraging artificial intelligence to reduce diagnostic errors in emergency medicine: Challenges, opportunities, and future directions
- PMID: 39676165
- PMCID: PMC11921089
- DOI: 10.1111/acem.15066
Leveraging artificial intelligence to reduce diagnostic errors in emergency medicine: Challenges, opportunities, and future directions
Abstract
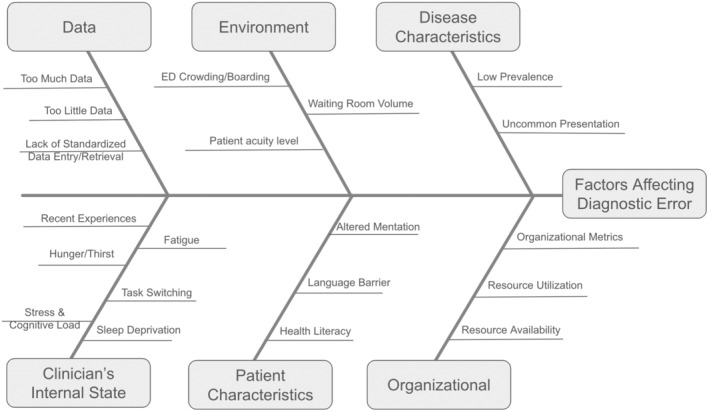
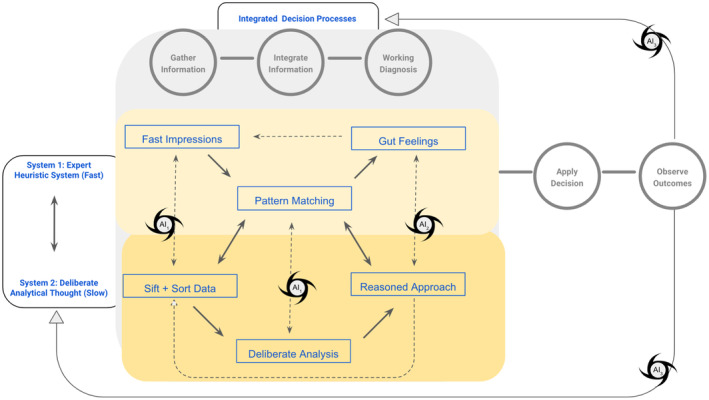
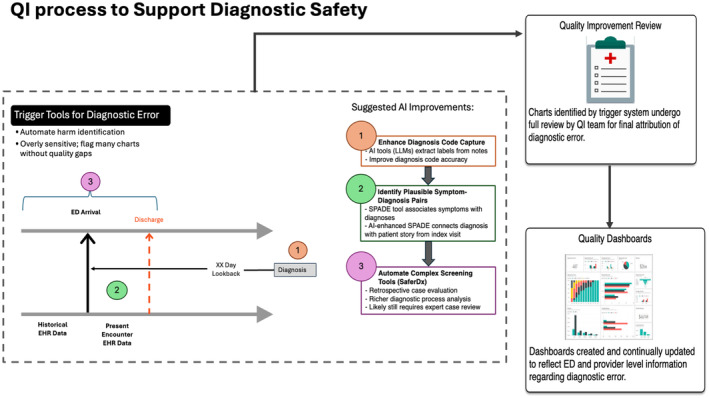
Diagnostic errors in health care pose significant risks to patient safety and are disturbingly common. In the emergency department (ED), the chaotic and high-pressure environment increases the likelihood of these errors, as emergency clinicians must make rapid decisions with limited information, often under cognitive overload. Artificial intelligence (AI) offers promising solutions to improve diagnostic errors in three key areas: information gathering, clinical decision support (CDS), and feedback through quality improvement. AI can streamline the information-gathering process by automating data retrieval, reducing cognitive load, and providing clinicians with essential patient details quickly. AI-driven CDS systems enhance diagnostic decision making by offering real-time insights, reducing cognitive biases, and prioritizing differential diagnoses. Furthermore, AI-powered feedback loops can facilitate continuous learning and refinement of diagnostic processes by providing targeted education and outcome feedback to clinicians. By integrating AI into these areas, the potential for reducing diagnostic errors and improving patient safety in the ED is substantial. However, successfully implementing AI in the ED is challenging and complex. Developing, validating, and implementing AI as a safe, human-centered ED tool requires thoughtful design and meticulous attention to ethical and practical considerations. Clinicians and patients must be integrated as key stakeholders across these processes. Ultimately, AI should be seen as a tool that assists clinicians by supporting better, faster decisions and thus enhances patient outcomes.
© 2024 The Author(s). Academic Emergency Medicine published by Wiley Periodicals LLC on behalf of Society for Academic Emergency Medicine.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- National Academies of Sciences, Engineering, and Medicine, Institute of Medicine, Board on Health Care Services, Committee on Diagnostic Error in Health Care . Improving Diagnosis in Health Care. National Academies Press; 2016.
-
- Board on Health Care Services . Committee on Diagnostic Error in Health Care. Improving Diagnosis in Health Care. National Academies Press; 2016. - PubMed
-
- Iyengar SS, Lepper MR. When choice is demotivating: can one desire too much of a good thing? In: Lichtenstein S, Slovic P, eds. The Construction of Preference. Cambridge University Press; 2006:300‐322.
-
- Cook DA, Sherbino J, Durning SJ. Management reasoning: beyond the diagnosis. JAMA. 2018;319(22):2267‐2268. - PubMed
-
- Patel JJ, Bergl PA. Diagnostic vs management reasoning. JAMA. 2018;320(17):1818. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
