

A Salivary Clear Cell Tumor With an Unclear Diagnosis: A Report of a Rare Case
- PMID: 39677248
- PMCID: PMC11646157
- DOI: 10.7759/cureus.73656
A Salivary Clear Cell Tumor With an Unclear Diagnosis: A Report of a Rare Case
Abstract
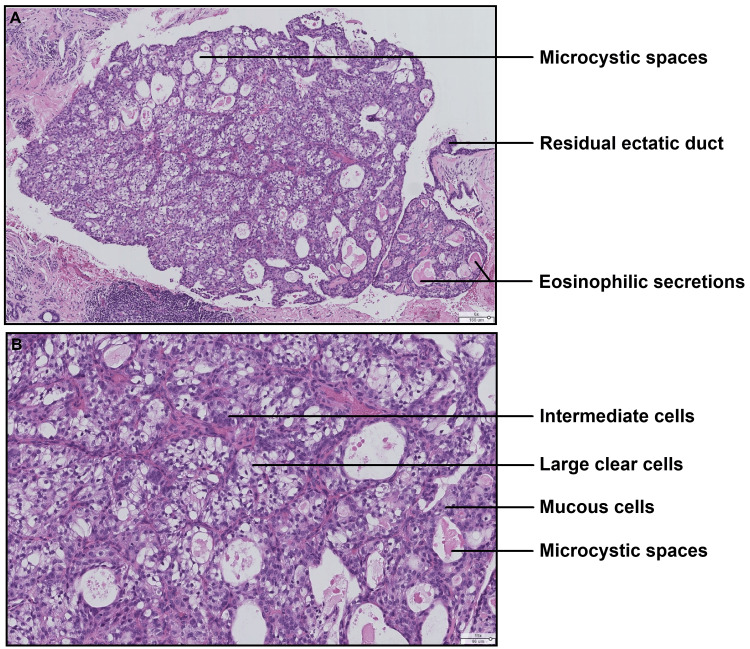
The histopathological diagnosis of salivary tumors is considered complex, due to their histological, phenotypic, and genotypic diversity. There are numerous tumors with morphological and/or immunohistochemical aspects that are superimposable but require very different treatment. In this context, salivary lesions containing clear cells are numerous and form part of the diagnostic challenges. We present the case of a 63-year-old woman with a tumor of the accessory salivary glands of the palate, with a predominant clear cell contingent. The aim of this paper is to report a case of a clear cell salivary tumor and to detail the difficulties of differential diagnosis, highlighting new data in the literature and the role of molecular biology.
Keywords: clear cells; malignant salivary gland tumor; minor salivary gland; oral cavity; salivary gland tumor.
Copyright © 2024, Strokov et al.
Conflict of interest statement
Human subjects: Consent for treatment and open access publication was obtained or waived by all participants in this study. Conflicts of interest: In compliance with the ICMJE uniform disclosure form, all authors declare the following: Payment/services info: All authors have declared that no financial support was received from any organization for the submitted work. Financial relationships: All authors have declared that they have no financial relationships at present or within the previous three years with any organizations that might have an interest in the submitted work. Other relationships: All authors have declared that there are no other relationships or activities that could appear to have influenced the submitted work.
Figures




References
-
- Bishop JA, Thompson LD, Wakely PE, Weinreb I. Arlington (VA): American Registry of Pathology; 2021. Tumors of the salivary glands.
-
- Head and neck tumours: WHO classification of tumours. Geneva, Switzerland: World Health Organization; 2024.
-
- The evolving role of molecular pathology in the diagnosis of salivary gland tumours with potential pitfalls. Kaur K, Mehta S, Vanik S, et al. Eur Arch Otorhinolaryngol. 2022;279:3769–3783. - PubMed
Publication types
LinkOut - more resources
Full Text Sources