

This is a preprint.
Induced B-Cell Receptor Diversity Predicts PD-1 Blockade Immunotherapy Response
- PMID: 39677742
- PMCID: PMC11643026
- DOI: 10.1101/2024.12.03.626669
Induced B-Cell Receptor Diversity Predicts PD-1 Blockade Immunotherapy Response
Update in
-
Induced B cell receptor diversity predicts PD-1 blockade immunotherapy response.Proc Natl Acad Sci U S A. 2025 May 6;122(18):e2501269122. doi: 10.1073/pnas.2501269122. Epub 2025 May 2. Proc Natl Acad Sci U S A. 2025. PMID: 40314973 Free PMC article.
Abstract
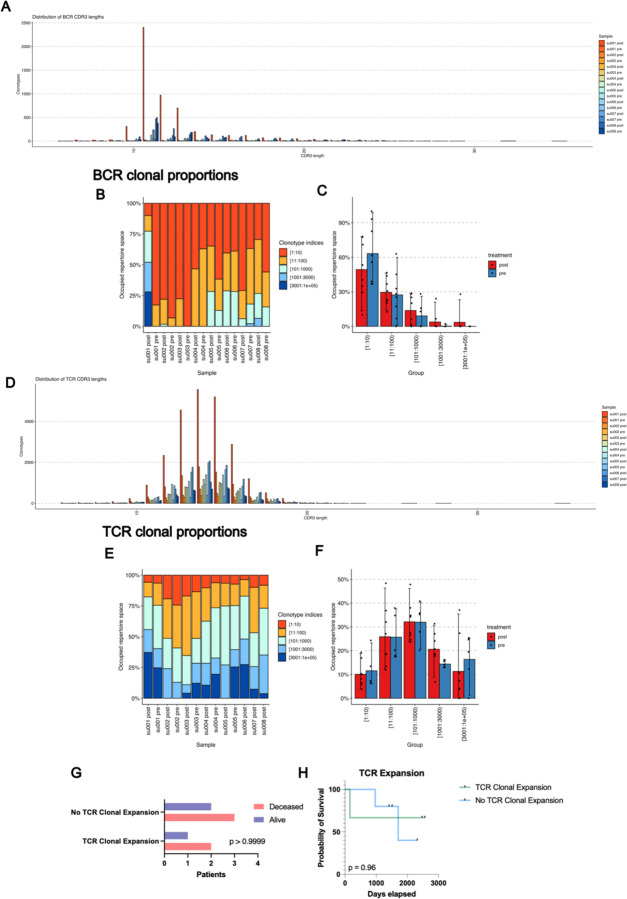
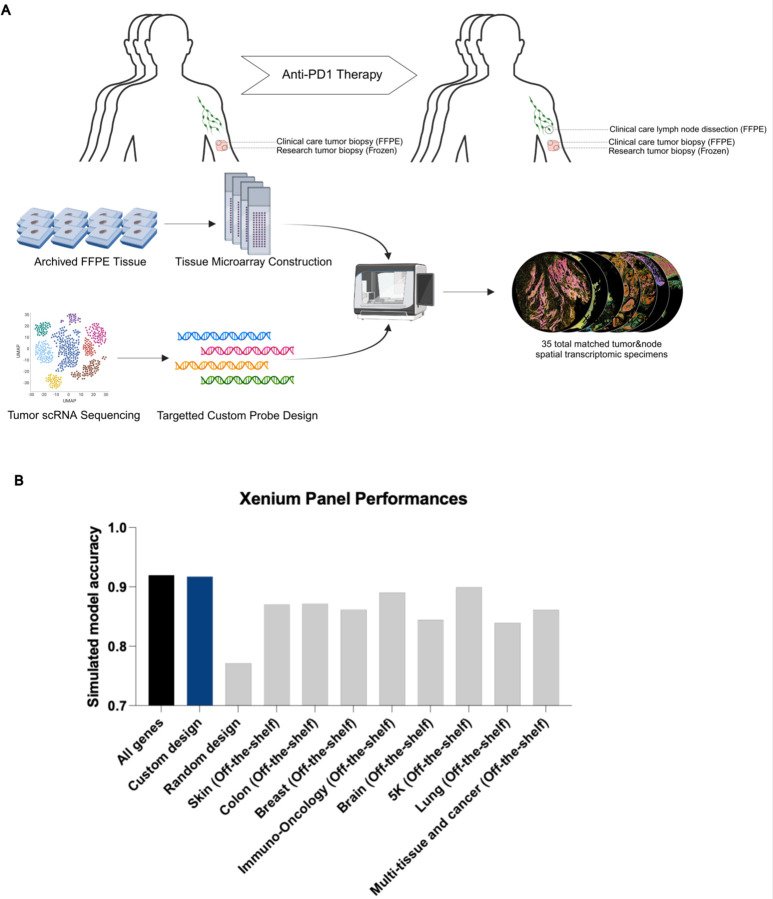
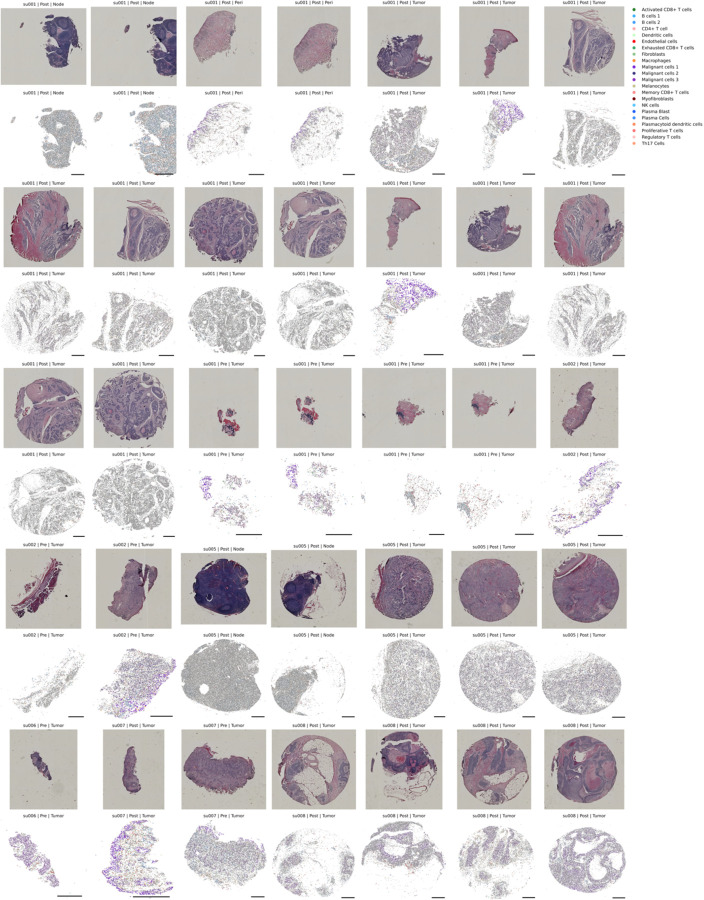
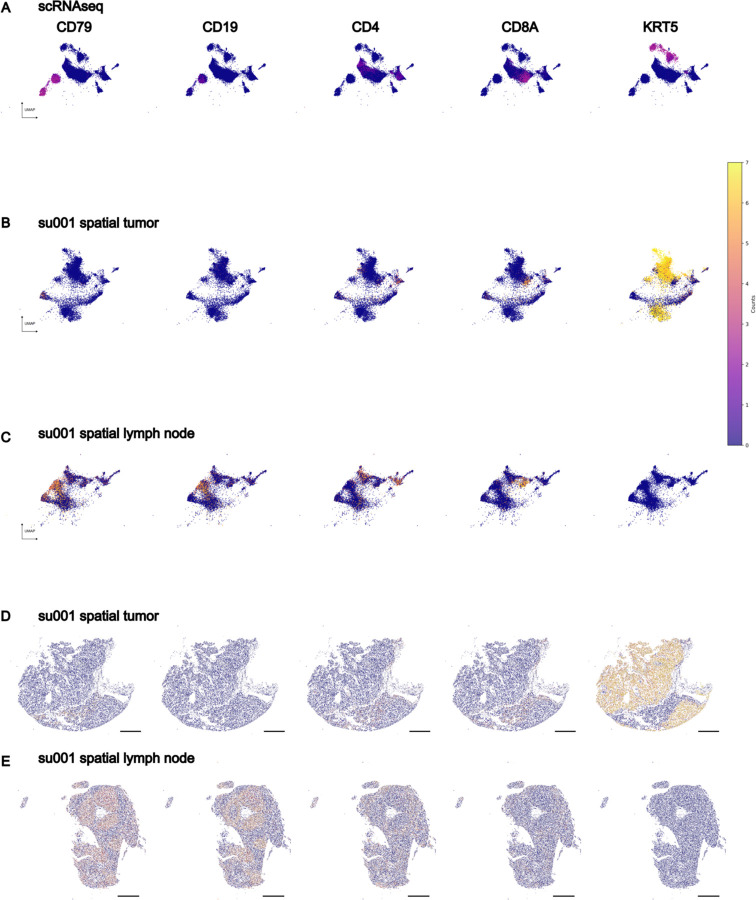
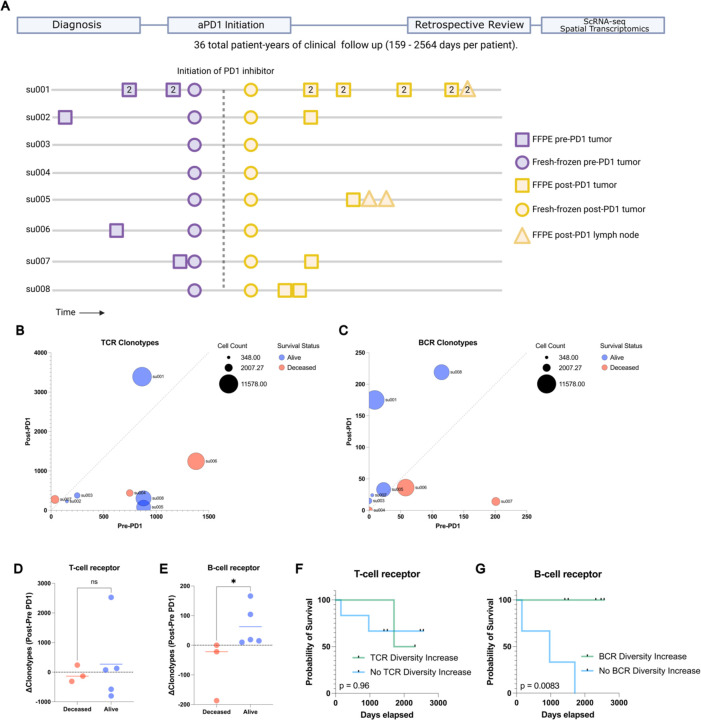
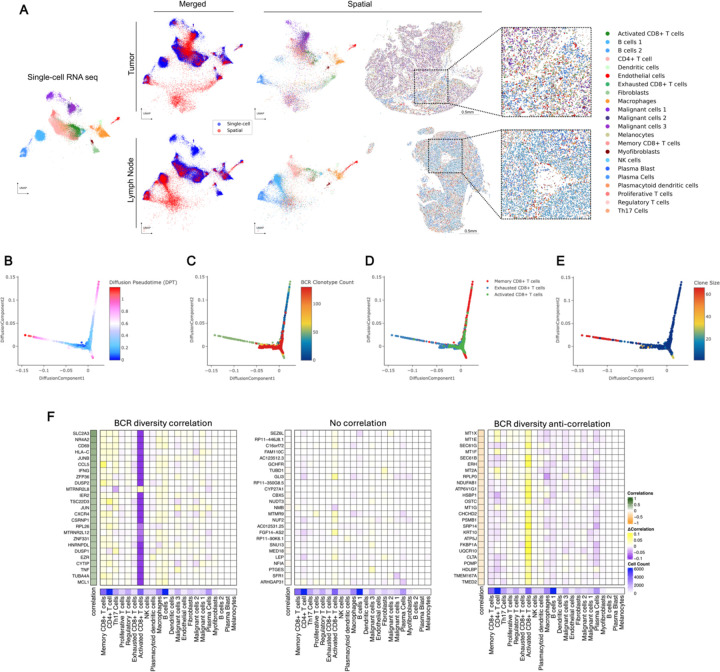
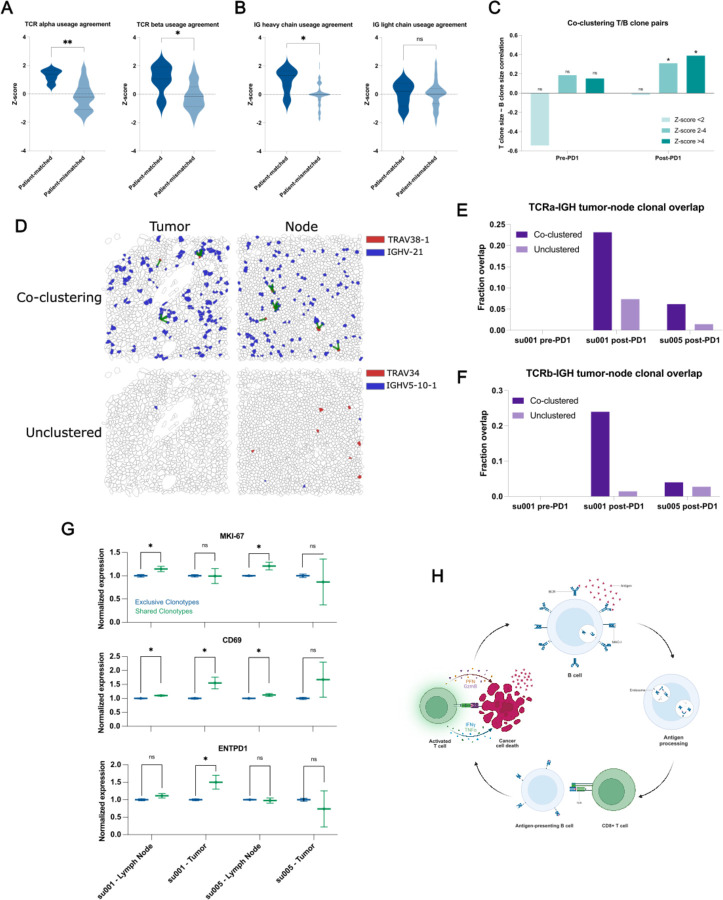
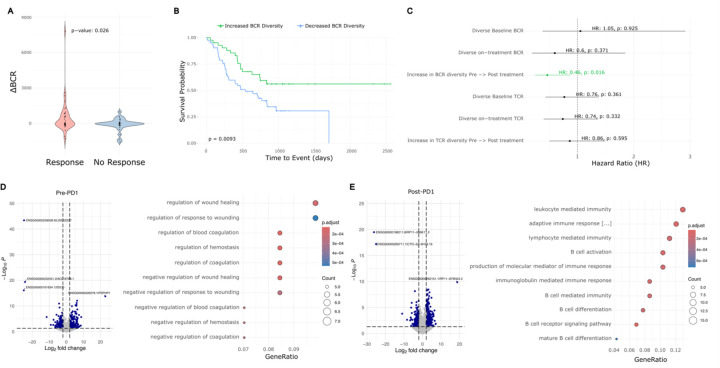
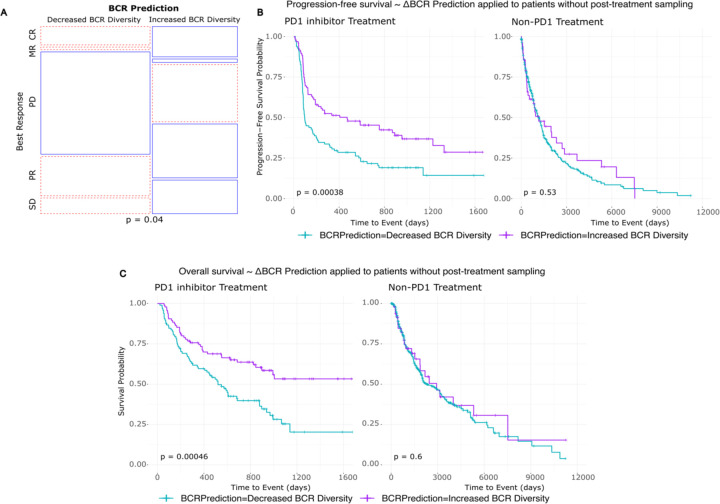
Immune checkpoint inhibitors such as anti-PD-1 antibodies (aPD1) can be effective in treating advanced cancers. However, many patients do not respond and the mechanisms underlying these differences remain incompletely understood. In this study, we profile a cohort of patients with locally-advanced or metastatic basal cell carcinoma undergoing aPD-1 therapy using single-cell RNA sequencing, high-definition spatial transcriptomics in tumors and draining lymph nodes, and spatial immunoreceptor profiling, with long-term clinical follow-up. We find that successful responses to PD-1 inhibition are characterized by an induction of B-cell receptor (BCR) clonal diversity after treatment initiation. These induced BCR clones spatially co-localize with T-cell clones, facilitate their activation, and traffic alongside them between tumor and draining lymph nodes to enhance tumor clearance. Furthermore, we validated aPD1-induced BCR diversity as a predictor of clinical response in a larger cohort of glioblastoma, melanoma, and head and neck squamous cell carcinoma patients, suggesting that this is a generalizable predictor of treatment response across many types of cancers. We discover that pre-treatment tumors harbor a characteristic gene expression signature that portends a higher probability of inducing BCR clonal diversity after aPD-1 therapy, and we develop a machine learning model that predicts PD-1-induced BCR clonal diversity from baseline tumor RNA sequencing. These findings underscore a dynamic role of B cell diversity during immunotherapy, highlighting its importance as a prognostic marker and a potential target for intervention in non-responders.
Figures
References
-
- Cabrita R., Lauss M., Sanna A., Donia M., Skaarup Larsen M., Mitra S., Johansson I., Phung B., Harbst K., Vallon-Christersson J., van Schoiack A., Lövgren K., Warren S., Jirström K., Olsson H., Pietras K., Ingvar C., Isaksson K., Schadendorf D., … Jönsson G. (2020). Tertiary lymphoid structures improve immunotherapy and survival in melanoma. Nature, 577(7791). 10.1038/s41586-019-1914-8 - DOI - PubMed
-
- Chaft J. E., Oezkan F., Kris M. G., Bunn P. A., Wistuba I. I., Kwiatkowski D. J., Owen D. H., Tang Y., Johnson B. E., Lee J. M., Lozanski G., Pietrzak M., Seweryn M., Byun W. Y., Schulze K., Nicholas A., Johnson A., Grindheim J., Hilz S., … Blasberg J. D. (2022). Neoadjuvant atezolizumab for resectable non-small cell lung cancer: an open-label, single-arm phase II trial. Nature Medicine, 28(10). 10.1038/s41591-022-01962-5 - DOI - PMC - PubMed
-
- Chang T.-G., Spathis A., Schäffer A. A., Gavrielatou N., Kuo F., Jia D., Mukherjee S., Sievers C., Economopoulou P., Anastasiou M., Moutafi M., Pal L. R., Vos J., Lee A. S., Lam S., Zhao K., Jiang P., Allen C. T., Foukas P., … Ruppin E. (2024). Tumor and Blood B Cell Abundance Outperforms Established Immune Checkpoint Blockade Response Prediction Signatures in Head and Neck Cancer. Annals of Oncology. 10.1016/j.annonc.2024.11.008 - DOI - PMC - PubMed
-
- Cloughesy T. F., Mochizuki A. Y., Orpilla J. R., Hugo W., Lee A. H., Davidson T. B., Wang A. C., Ellingson B. M., Rytlewski J. A., Sanders C. M., Kawaguchi E. S., Du L., Li G., Yong W. H., Gaffey S. C., Cohen A. L., Mellinghoff I. K., Lee E. Q., Reardon D. A., … Prins R. M. (2019). Neoadjuvant anti-PD-1 immunotherapy promotes a survival benefit with intratumoral and systemic immune responses in recurrent glioblastoma. Nature Medicine, 25(3). 10.1038/s41591-018-0337-7 - DOI - PMC - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources