

Clinical-Radiomics Nomogram Model Based on CT Angiography for Prediction of Intracranial Aneurysm Rupture: A Multicenter Study
- PMID: 39678712
- PMCID: PMC11645942
- DOI: 10.2147/JMDH.S491697
Clinical-Radiomics Nomogram Model Based on CT Angiography for Prediction of Intracranial Aneurysm Rupture: A Multicenter Study
Abstract
Objective: Risk estimation of intracranial aneurysm rupture is critical in determining treatment strategy. There is a scarcity of multicenter studies on the predictive power of clinical-radiomics models for aneurysm rupture. This study aims to develop a clinical-radiomics model and explore its additional value in the discrimination of aneurysm rupture.
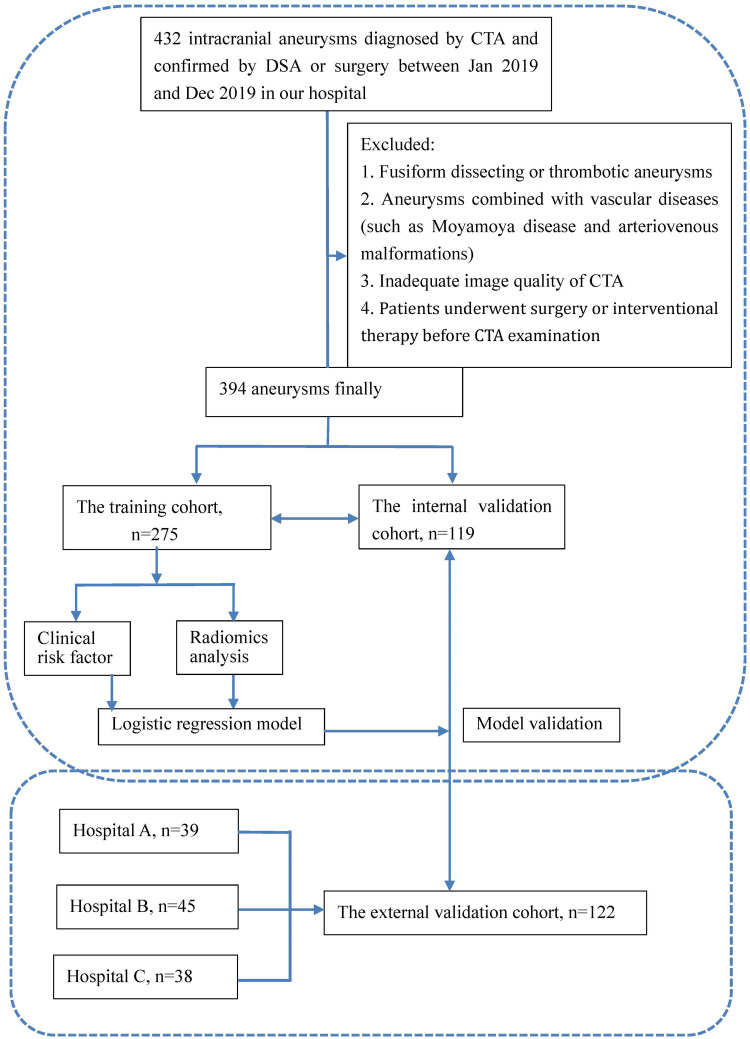
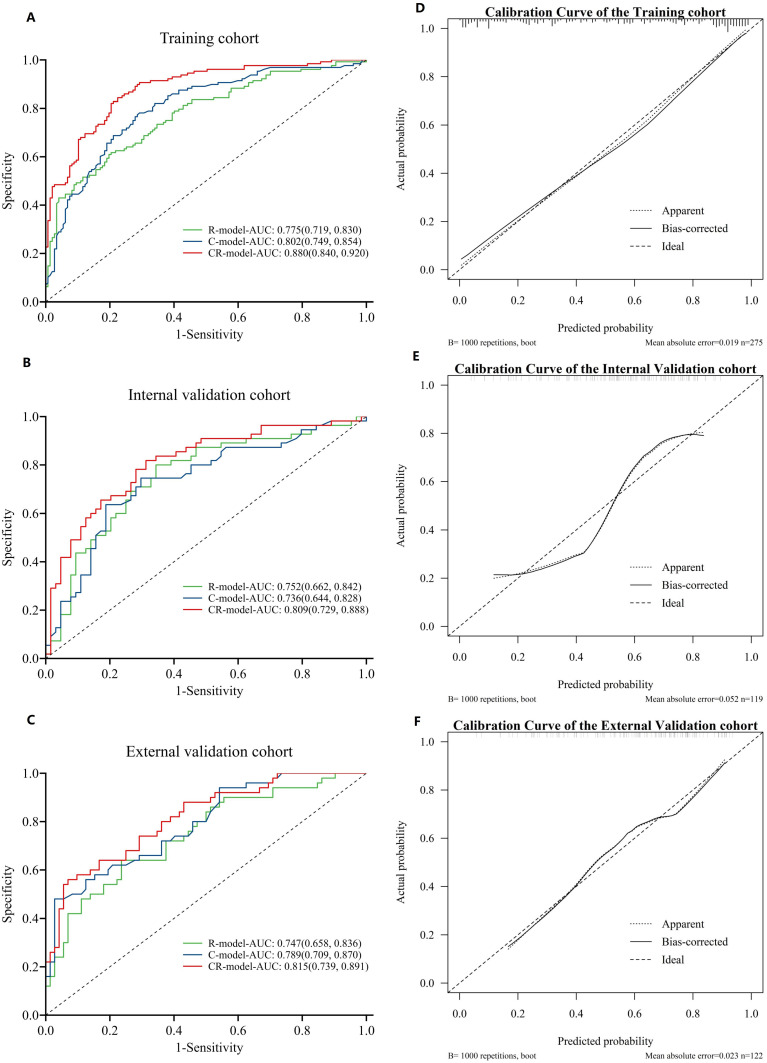
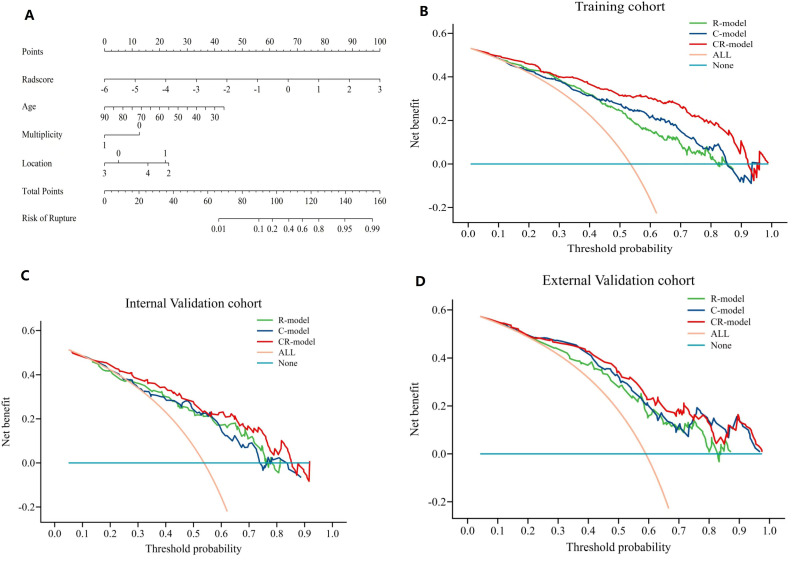
Methods: A total of 516 aneurysms, including 273 (52.9%) with ruptured aneurysms, were retrospectively enrolled from four hospitals between January 2019 and August 2020. Relevant clinical features were collected, and radiomic characteristics associated with aneurysm were extracted. Subsequently, three models, including a clinical model, a radiomics model, and a clinical-radiomics model were constructed using multivariate logistic regression analysis to effectively classify aneurysm rupture. The performance of models was analyzed through operating characteristic curves, decision curve, and calibration curves analysis. Different models' comparison used DeLong tests. To offer an understandable and intuitive scoring system for assessing rupture risk, we developed a comprehensive nomogram based on the developed model.
Results: Three clinical risk factors and fourteen radiomics features were explored to establish three models. The area under the receiver operating curve (AUC) for the radiomics model was 0.775 (95% CI,0.719-0.830), 0.752 (95% CI,0.663-0.841), 0.747 (95% CI,0.658-0.835) in the training, internal and external test datasets, respectively. The AUC for clinical model was 0.802 (95% CI, 0.749-0.854), 0.736 (95% CI, 0.644-0.828), 0.789 (95% CI, 0.709-0.870) in these three sets, respectively. The clinical-radiomics model showed an AUC of 0.880 (95% CI,0.840-0.920), 0.807 (95% CI,0.728-0.887), 0.815 (95% CI,0.740-0.891) in three datasets respectively. Compared with the radiomics and clinical models, the clinical-radiomics model demonstrated better diagnostic performance (DeLong' test P < 0.05).
Conclusion: The clinical-radiomics model represents a promising approach for predicting rupture of intracranial aneurysms.
Keywords: computed tomography angiography; intracranial aneurysm; nomograms; radiomics; rupture.
© 2024 Jia et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures
References
LinkOut - more resources
Full Text Sources
