

Emphysematous pancreatitis: Diagnosis, treatment, and prognosis
- PMID: 39679309
- PMCID: PMC11612709
- DOI: 10.3748/wjg.v30.i46.4929
Emphysematous pancreatitis: Diagnosis, treatment, and prognosis
Abstract
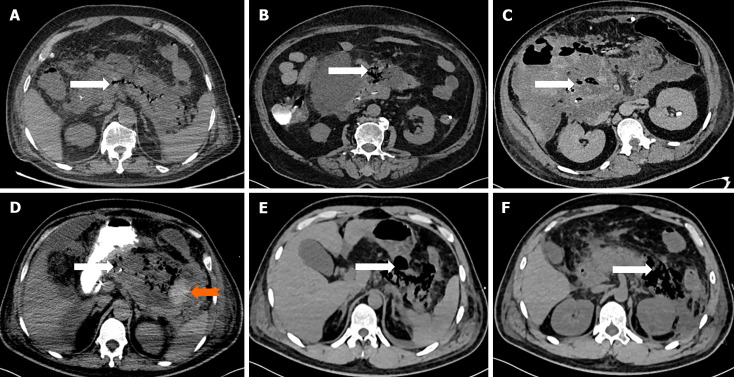
Background: Emphysematous pancreatitis (EP) is a rare, severe form of acute necrotizing pancreatitis characterized by gas in pancreatic or peripancreatic tissue, with a high mortality rate.
Aim: To assess the diagnosis, treatment, and outcomes of EP through a series of case studies.
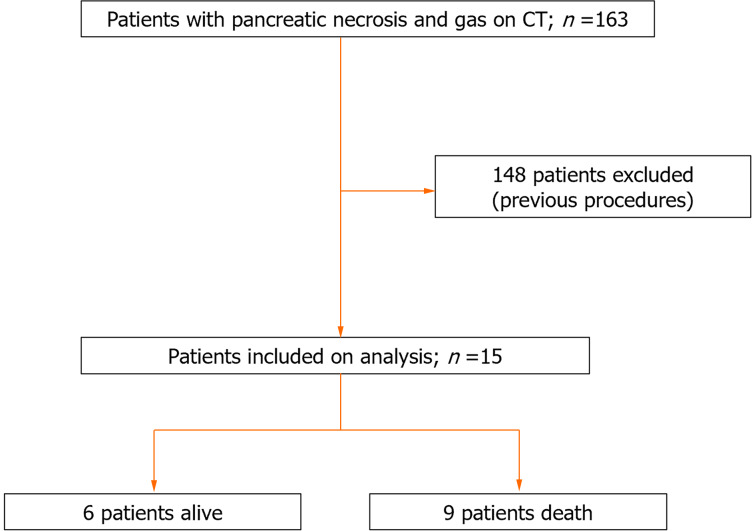
Methods: This case series was conducted in intensive care units at the Second Affiliated Hospital of Anhui Medical University. Patients were included if they were diagnosed with pancreatic necrosis and gas via computed tomography from June 2018 to June 2024. Patients were categorized into early and late EP groups based on the timing of the appearance of the bubble sign and into extensive and common types based on the distribution range of the bubble sign. The data recorded included sex, age, aetiology, Acute Physiology and Chronic Health Evaluation II score, Sequential Organ Failure Assessment score, Bedside Index for Severity in Acute Pancreatitis score, subtype, gas distribution extent, aetiological diagnostic basis, pathogen categories, intervention measures, and prognosis.
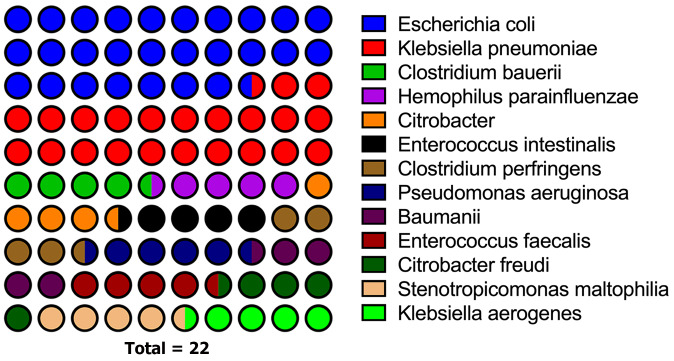
Results: Among the 15 patients, 66.7% had a biliary aetiology and extensive type of EP, 47.1% had early-onset EP, and 73.3% had confirmed aetiological evidence [6 based on bacterial culture, 4 based on both routine culture and next-generation sequencing (NGS), and 1 solely based on NGS]. The common pathogens were Escherichia coli and Klebsiella pneumoniae. Six patients survived. Among the 2 patients who did not undergo percutaneous drainage or surgical treatment, 1 survived. Of the 6 patients who underwent percutaneous drainage, 2 survived, 2 survived after subsequent surgery, and 2 died without surgery. Among the 6 patients who underwent surgery alone, 5 died and 1 survived. Among the early-onset EP patients, 4 survived; among the late-onset EP patients, 2 survived. Among the common EP types, 4 survived; among the extensive EP types, only 1 survived.
Conclusion: The mortality rate among patients with EP is considerable, and NGS enhances pathogen identification accuracy. Despite the debate on conservative vs surgical management, the STEP-UP strategy remains viable. Aggressive antimicrobial therapy, early percutaneous catheter drainage, and other minimally invasive interventions, along with delayed surgical intervention, may improve patient prognosis.
Keywords: Diagnosis; Emphysematous pancreatitis; Next-generation sequencing; Prognosis; Treatment.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: All the authors report no relevant conflicts of interest for this article.
Figures
References
-
- Baron TH, DiMaio CJ, Wang AY, Morgan KA. American Gastroenterological Association Clinical Practice Update: Management of Pancreatic Necrosis. Gastroenterology. 2020;158:67–75.e1. - PubMed
-
- Boxhoorn L, Voermans RP, Bouwense SA, Bruno MJ, Verdonk RC, Boermeester MA, van Santvoort HC, Besselink MG. Acute pancreatitis. Lancet. 2020;396:726–734. - PubMed
-
- Forsmark CE, Vege SS, Wilcox CM. Acute Pancreatitis. N Engl J Med. 2016;375:1972–1981. - PubMed
-
- Waller A, Long B, Koyfman A, Gottlieb M. Acute Pancreatitis: Updates for Emergency Clinicians. J Emerg Med. 2018;55:769–779. - PubMed
-
- Wig JD, Kochhar R, Bharathy KG, Kudari AK, Doley RP, Yadav TD, Kalra N. Emphysematous pancreatitis. Radiological curiosity or a cause for concern? JOP. 2008;9:160–166. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
