

Field-testing the explicit diagnostic criteria for transient ischemic attack: a diagnostic accuracy study
- PMID: 39680237
- PMCID: PMC11649740
- DOI: 10.1007/s00415-024-12733-2
Field-testing the explicit diagnostic criteria for transient ischemic attack: a diagnostic accuracy study
Abstract
Background and aim: Explicit diagnostic criteria for transient ischemic attack (TIA) (EDCT) have been recently proposed based on the assumption, that a migraine aura-like symptom is not typical for a TIA. However, migraine-like symptoms have been unexpectedly frequent in patients with confirmed ischemic stroke. This cross-sectional study aimed to field-test the EDCT to distinguish transient neurological symptoms caused by cerebral infarction from those caused by migraine aura.
Methods: The sensitivity, specificity, positive and negative predictive values of the EDCT score were calculated in samples of patients with (i) transient symptoms caused by cerebral infarction confirmed by imaging and (ii) patients with migraine with aura diagnosed according to the International Classification of Headache Disorders 3rd edition. Sensitivity, specificity, positive and negative predictive values of the original and modified EDCT were calculated, as well as area under the curve adjusted for age and sex using the logistic regression method.
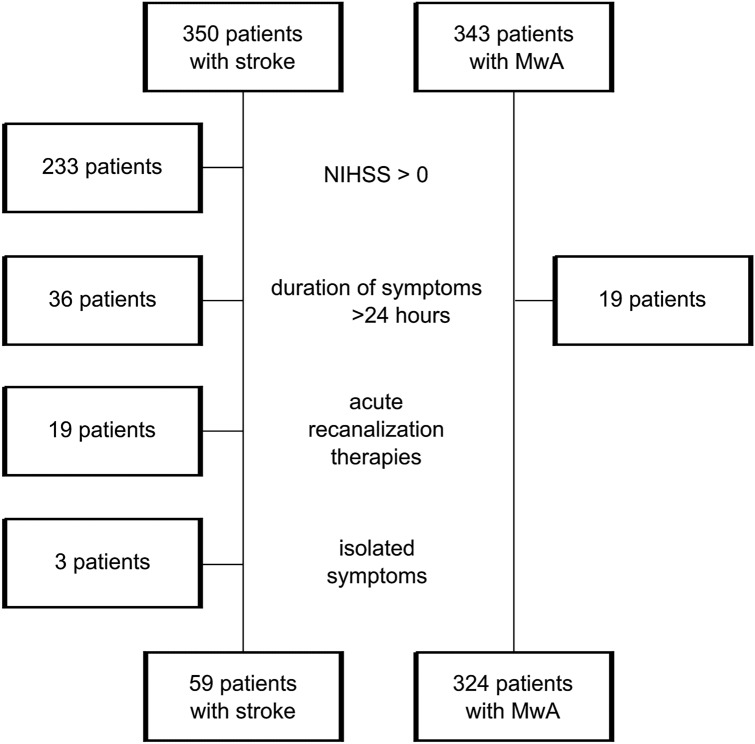
Results: The study population included 59 patients with cerebral infarction and 324 patients with migraine with aura. The median age of the stroke group was 72 (IQR 61-81) and of the migraine group 39 (IQR 29-53). There were 36 (61%) men in the stroke group and 221 (68%) women in the migraine group. For the detection of TIA with imaging-proven cerebral infarction, the original EDCT had a sensitivity of 90% (95%CI 79-96), a specificity 77% (95%CI 72-82), a positive predictive value of 42% (95%CI 33-51), and the negative predictive value 98% (95% CI 95-99). For the modified EDCT, the sensitivity was 81% (95%CI 69-90), the specificity 97% (95%CI 94-98), the positive predictive value 81% (95%CI 69-90), and the negative predictive value 97% (95%CI 94-98).
Conclusions: The original and modified EDCT criteria miss up to 1 of 10 and 1 of 5 patients, respectively, with transient symptoms due to cerebral infarction. However, the modified EDCT criteria are more specific but less sensitive in detection of ischemic events. The optimal combination of clinical markers to reliably distinguish TIA from migraine aura remains to be found.
Keywords: Migraine aura; accuracy; ischemic stroke; score; transient ischemic attack.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Conflicts of interest: AS received research support from Swiss Heart Foundation and TEVA pharmaceuticals. MB reports research support from the Department of Neurology, Inselspital, and the University of Bern, Switzerland. TRM reports grants from the Bangerter-Rhyner Foundation, the Baasch-Medicus Foundation, the University of Bern, the Swiss National Science Foundation and the Swiss Heart Foundation. MA reports speaker honoraria from Astra Zeneca, Bayer, Covidien, Medtronic, Sanofi and honoraria for scientific advisory boards from Amgen, Bayer, BMS, Daiichi Sankyo, Medtronic, Pfizer, and research funding from the Swiss National Science Foundation (SNSF), and the Swiss Heart Foundation (SHF). UF reports financial support for the SWIFT DIRECT trial (Medtronic), research grants from Medtronic BEYOND SWIFT registry, SNSF, SHF, consulting fees from Medtronic, Stryker and CSL Behring (fees paid to institution); membership of a Data Safety Monitoring Board for the IN EXTREMIS trial and TITAN trial and Portola (Alexion) Advisory board (fees paid to institution). HPM was neurology principal investigator of the PC-Trial, was member of the steering committee of the PRIMA Trial, and reports consultancy fees from Medtronic, Stryker and Cerenovus. JO owns stock in Novo Nordisk, Moberg Pharma and Cephagenix. SJ reports grants from the Swiss National Science Foundation and the Swiss Heart Foundation. CJS reports consulting, Advisory Boards, Speaker, Travel Support for/from Abbvie, Allergan, Almirall, Amgen, Eli Lilly, Grnenthal, Lundbeck, MindMed, Novartis, Pfizer and TEVA Pharmaceuticals. All other authors have nothing to disclose.
Figures
References
-
- Easton JD, Saver JL, Albers GW, et al; American Heart Association; American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; Interdisciplinary Council on Peripheral Vascular Disease. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease (2009) The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke 40(6):2276–2293 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
