

Exploration of simultaneous transients between cerebral hemodynamics and the autonomic nervous system using windowed time-lagged cross-correlation matrices: a CENTER-TBI study
- PMID: 39680255
- PMCID: PMC11649841
- DOI: 10.1007/s00701-024-06375-6
Exploration of simultaneous transients between cerebral hemodynamics and the autonomic nervous system using windowed time-lagged cross-correlation matrices: a CENTER-TBI study
Abstract
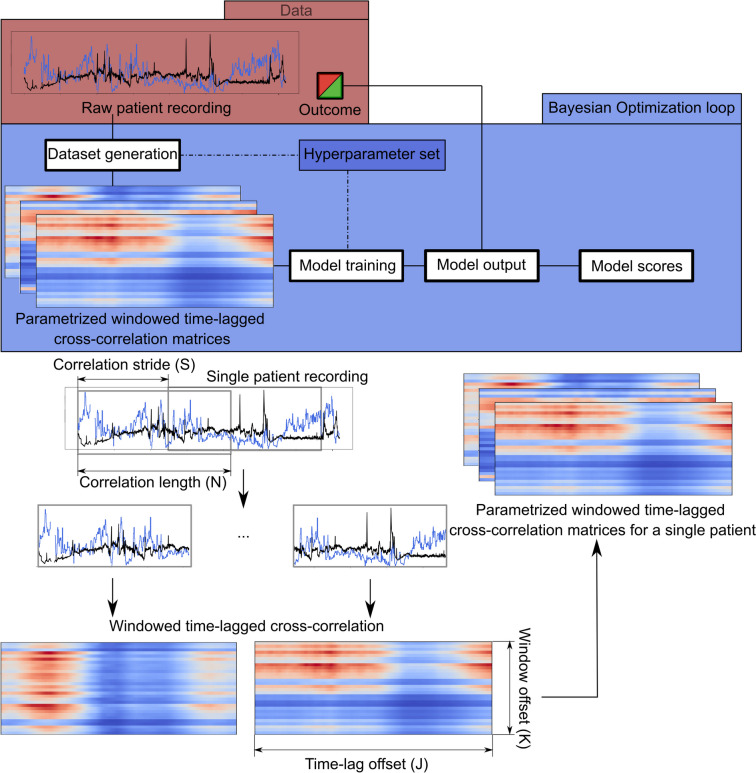
Background: Traumatic brain injury (TBI) can significantly disrupt autonomic nervous system (ANS) regulation, increasing the risk for secondary complications, hemodynamic instability, and adverse outcome. This retrospective study evaluated windowed time-lagged cross-correlation (WTLCC) matrices for describing cerebral hemodynamics-ANS interactions to predict outcome, enabling identifying high-risk patients who may benefit from enhanced monitoring to prevent complications.
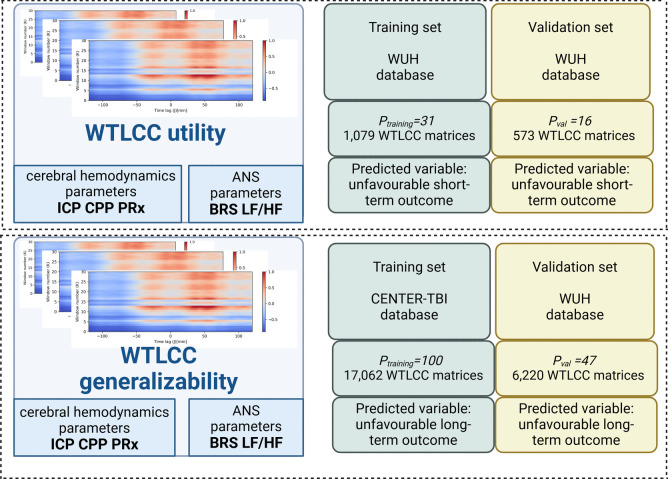
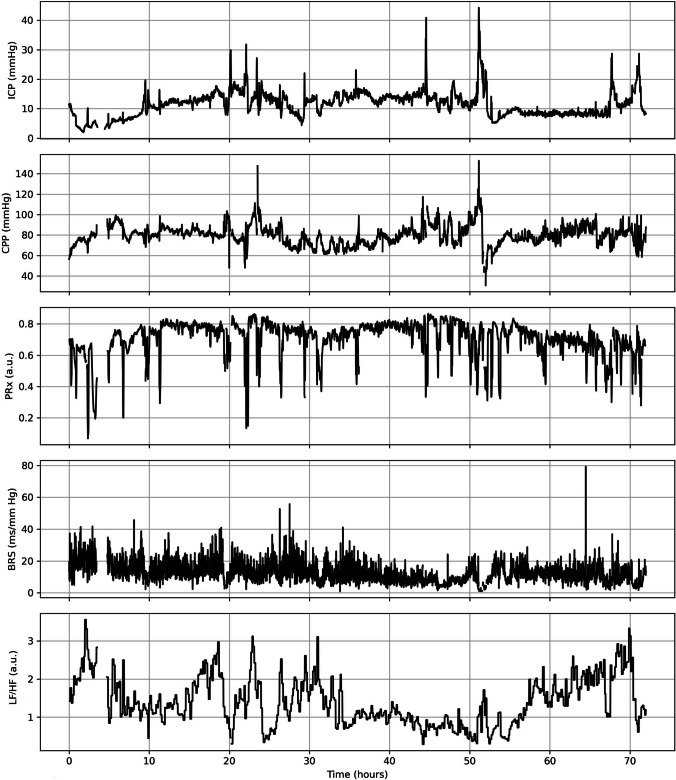
Methods: The first experiment aimed to predict short-term outcome using WTLCC-based convolution neural network models on the Wroclaw University Hospital (WUH) database (Ptraining = 31 with 1,079 matrices, Pval = 16 with 573 matrices). The second experiment predicted long-term outcome, training on the CENTER-TBI database (Ptraining = 100 with 17,062 matrices) and validating on WUH (Pval = 47 with 6,220 matrices). Cerebral hemodynamics was characterized using intracranial pressure (ICP), cerebral perfusion pressure (CPP), pressure reactivity index (PRx), while ANS metrics included low-to-high-frequency heart rate variability (LF/HF) and baroreflex sensitivity (BRS) over 72 h. Short-term outcome at WUH was assessed using the Glasgow Outcome Scale (GOS) at discharge. Long-term outcome was evaluated at 3 months at WUH and 6 months at CENTER-TBI using GOS and GOS-Extended, respectively. The XGBoost model was used to compare performance of WTLCC-based model and averaged neuromonitoring parameters, adjusted for age, Glasgow Coma Scale, major extracranial injury, and pupil reactivity in outcome prediction.
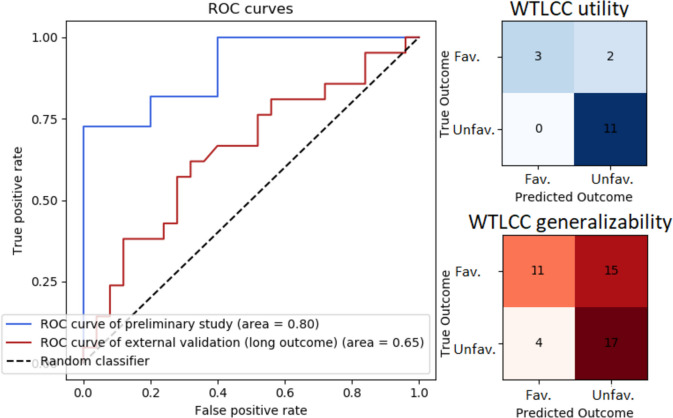
Results: For short-term outcome prediction, the best-performing WTLCC-based model used ICP-LF/HF matrices. It had an area under the curve (AUC) of 0.80, vs. 0.71 for averages of ANS and cerebral hemodynamics metrics, adjusted for clinical metadata. For long-term outcome prediction, the best-score WTLCC-based model used ICP-LF/HF matrices. It had an AUC of 0.63, vs. 0.66 for adjusted neuromonitoring parameters.
Conclusions: Among all neuromonitoring parameters, ICP and LF/HF signals were the most effective in generating the WTLCC matrices. WTLCC-based model outperformed adjusted neuromonitoring parameters in short-term but had moderate utility in long-term outcome prediction.
Keywords: Autonomic nervous system; Brain–heart coupling; Machine learning; Traumatic brain injury.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: The CENTER-TBI study (European Commission Grant 602150) was conducted in accordance with all relevant laws of the European Union that are directly applicable or of direct effects and all relevant laws of the country where the recruiting sites were located, including but not limited to, the relevant privacy and data protection laws and regulations (the “Privacy Law”), the relevant laws and regulations on the use of human materials, and all relevant guidance relating to clinical studies from time to time in force, including but not limited to, the ICH Harmonized Tripartite Guideline for Good Clinical Practice (CPMP/ICH/135/95) (“ICH GCP”) and the World Medical Association Declaration of Helsinki entitled “Ethical Principles for Medical Research Involving Human Subjects.” Informed consent by the patients and/or the legal representative/next of kin was obtained, according to the local legislations, for all patients recruited in the Core Dataset of CENTER-TBI and documented in the e-CRF. Ethical approval was obtained for each recruiting site from the appropriate local ethics committee, and the full list of approvals is available on the website: https://www.center-tbi.eu/project/ethical-approval . The retrospective analysis of data recorded at Wroclaw University Hospital (WUH) was approved by the bioethical committee of WUH (approval KB-133/2023). All volunteers were required to provide written consent before entering the study. The data were fully anonymised, and no data protection issues were involved. Consent for publication: The manuscript has not been submitted elsewhere or published elsewhere in whole or in part. Some of the results have been accepted as poster presentations for the 2024 meeting of the International NeuroTrauma Society (INTS) conference, which took place in September 2024 in Cambridge, UK. Figure 1 was created in BioRender.com. Competing interests: Prof. Robba received fees for lectures from Massimo and GE. Prof. Czosnyka has a financial interest in a part of the intensive care monitoring (ICM +) licensing fee.
Figures
References
-
- Ackland GL, Iqbal S, Paredes LG, Toner A, Lyness C, Jenkins N et al (2015) Individualised oxygen delivery targeted haemodynamic therapy in high-risk surgical patients: a multicentre, randomised, double-blind, controlled, mechanistic trial. Lancet Respir Med 3:33–41 - PubMed
-
- Åkerlund CAI, Holst A, Bhattacharyay S, Stocchetti N, Steyerberg E, Smielewski P et al (2024) Clinical descriptors of disease trajectories in patients with traumatic brain injury in the intensive care unit (CENTER-TBI): a multicentre observational cohort study. Lancet Neurol 23:71–80 - PubMed
-
- Barnaby D, Ferrick K, Kaplan DT, Shah S, Bijur P, Gallagher EJ (2002) Heart rate variability in emergency department patients with sepsis. Acad Emerg Med 9:661–670 - PubMed
-
- Behrens F, Moulder RG, Boker SM, Kret ME (2020) Quantifying physiological synchrony through windowed cross-correlation analysis: Statistical and theoretical considerations. bioRxiv, pp 1–53. 10.1101/2020.08.27.269746
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
