

Finerenone: a breakthrough mineralocorticoid receptor antagonist for heart failure, diabetes and chronic kidney disease
- PMID: 39680348
- PMCID: PMC11649598
- DOI: 10.1186/s43044-024-00586-z
Finerenone: a breakthrough mineralocorticoid receptor antagonist for heart failure, diabetes and chronic kidney disease
Abstract
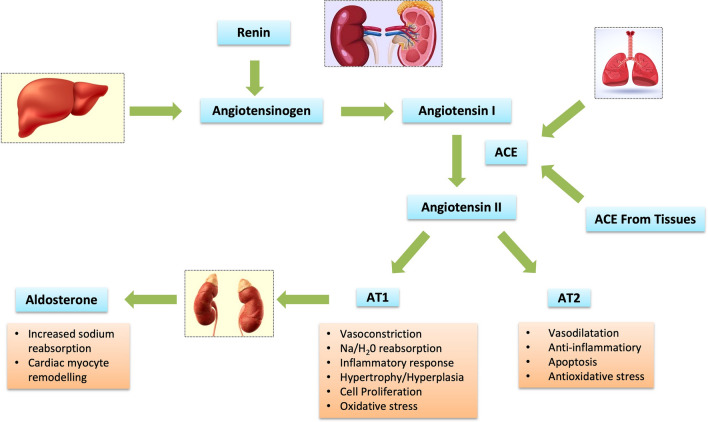
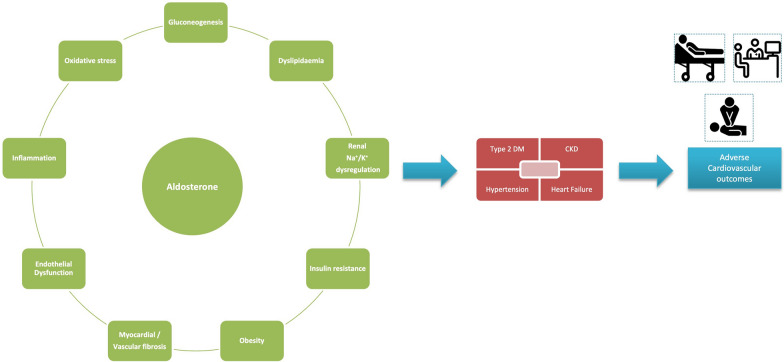
Background: Aldosterone is categorized as a mineralocorticoid hormone produced in the zona glomerulosa of the adrenal cortex. Aldosterone has considerable action in sodium and water retention along with cardiac remodeling, promoting fibrosis and these detrimental effects have been counteracted by mineralocorticoid receptors antagonists over time. Spironolactone, a non-selective steroidal MRA used extensively is potent but has serious adverse effects like gynecomastia and hyperkalemia. Eplerenone another second generation MRA, though non-steroidal and selective causes hyperkalemia and adversely effecting renal functions.
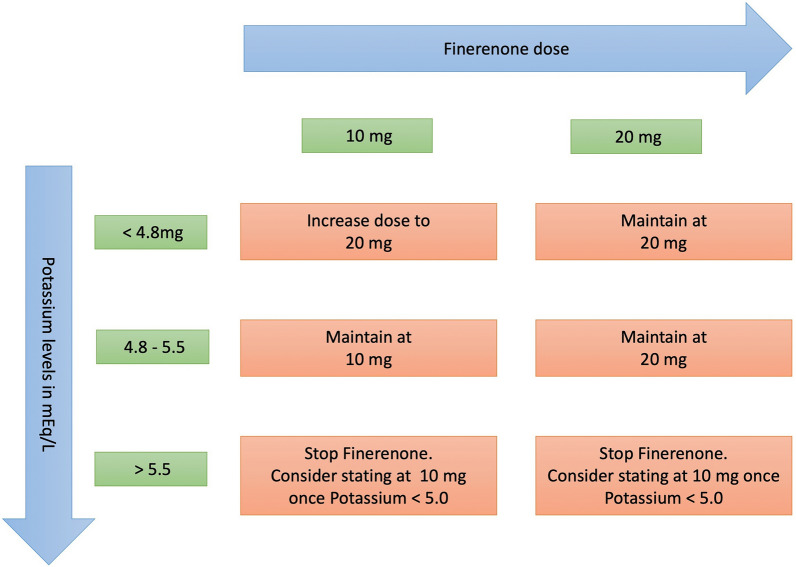
Main body: Recently Finerenone- a novel MRA has been introduced which is as potent like spironolactone with less adverse effects and improved cardiovascular outcomes particularly in chronic kidney failure with diabetes. The article reviews the physical and chemical properties of Finerenone and compares it with MRAs already in use, and then about the patient specific uses of Finerenone and future avenues of it. Finerenone is non-steroidal selective MRA, with promising results in improving the deterioration of renal functions in CKD with DM, reducing albuminuria with less hyperkalemia along with improvement in cardiovascular outcomes by reducing heart failure events.
Conclusion: Mineralocorticoid receptor antagonists have a proven role in preventing the adverse effects of RAAS pathway on heart, kidneys and blood vessels. Non-selective steroidal MRAs have potent action but by virtue of their non-selectivity associated with adverse effects like gynecomastia, hirsutism along with hyperkalemia Finerenone is novel non-steroidal & highly selective MRA, with promising results in halting the deterioration of renal functions in CKD with DM, reducing albuminuria, improvement in cardiovascular outcomes by reducing heart failure events albeit with less hyperkalemia. More randomized studies in dedicated HF patients are ongoing with Finerenone to prove it is worth in this sector with huge unmet need despite GDMT. Finerenone alleviates the risk of adverse renal and cardiac outcomes in patients with diabetes and CKD despite baseline medical therapy.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable.. Competing interests: The authors declare that they have no competing interests.
Figures
References
-
- Dutt M, Wehrle CJ, Jialal I. Physiology, adrenal gland. InStatPearls [Internet] 2022; StatPearls Publishing. - PubMed
-
- Scott JH, Menouar MA, Dunn RJ. Physiology, aldosterone. - PubMed
-
- Mantero F, Lucarelli G (2000) Aldosterone antagonists in hypertension and heart failure. Annales d’endocrinologie 61(1):52–60 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous