

Development of a latex microsphere-based lateral flow immunoassay for the diagnosis of schistosomiasis japonica
- PMID: 39680611
- PMCID: PMC11684761
- DOI: 10.1371/journal.pntd.0012742
Development of a latex microsphere-based lateral flow immunoassay for the diagnosis of schistosomiasis japonica
Abstract
Background: Zoonotic schistosomiasis, caused by Schistosoma japonicum, is prevalent in China, the Philippines and Indonesia. Rapid point-of-care (POC) diagnostics are attractive and promising tools for evaluating the efficacy of intervention strategies for schistosomiasis control.
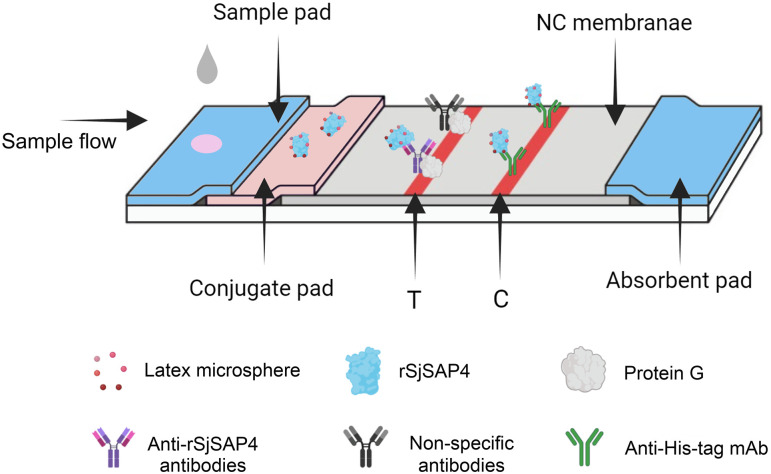
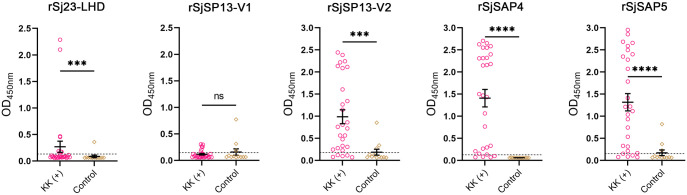
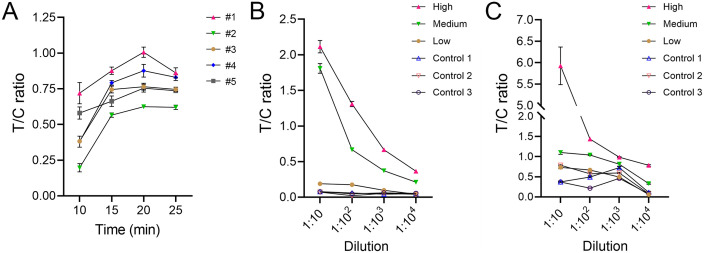
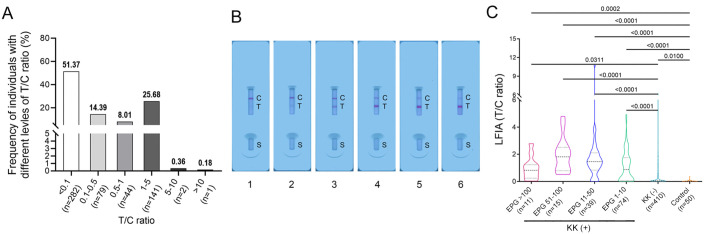
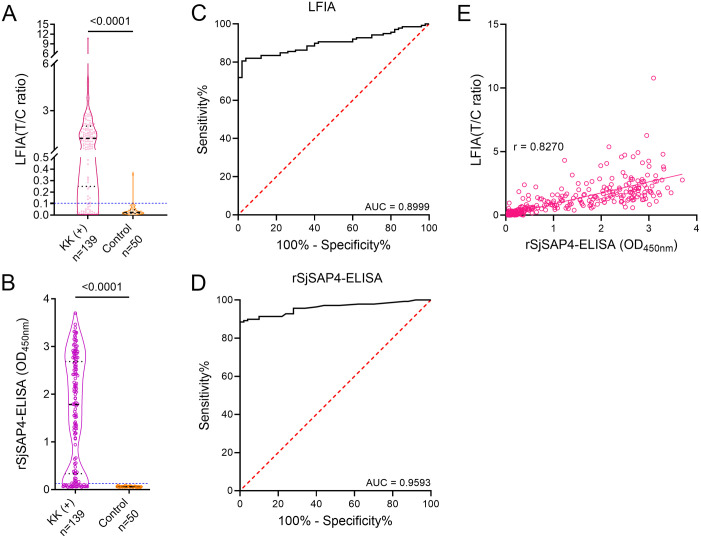
Methodology: The diagnostic potential of five recombinant antigens was tested by enzyme-linked immunosorbent assay (ELISA) using sera from individuals with positive Kato-Katz (KK) results for S. japonicum (n = 28) and non-endemic controls (n = 12). A latex microsphere (LM)-based lateral flow immunoassay (LFIA) incorporating the recombinant SjSAP4 (rSjSAP4) was developed for the diagnosis of schistosomiasis japonica. The test conditions including diluent, dilution factor and reaction time, were optimised for the developed LFIA. Under the optimised conditions, serum samples from individuals living in a barangay endemic for S. japonicum (n = 549) and non-endemic controls (n = 50) were tested with the established LFIA cassettes. The results were imaged by a smartphone and analysed by the ImageJ program. The intensity ratio of the test line to the control line (T/C ratio) was calculated for each cassette.
Main findings: ELISA confirmed that rSjSAP4 was the optimal candidate for serological diagnosis of schistosomiasis japonica. Under optimal testing conditions, the developed LFIA strips had a sensitivity of 80.6% and a specificity of 98.0% at a cut-off T/C ratio of 0.1031. Moreover, the results of the LM-based LFIA was positively correlated with those obtained from the rSjSAP4-ELISA (r = 0.8270, 95% CI, 0.7990-0.8514; p < 0.0001). The schistosomiasis prevalence determined by the LFIA strips was about 1.8 times greater than that obtained with the 6-slide KK procedure performed on three stool samples.
Conclusions/significance: The developed LFIA represents a POC diagnostic tool that is suitable for onsite screening of human S. japonicum infection with minimal equipment needed. The established immunochromatographic assay complies with most of the WHO's ASSURED criteria for POC diagnostics.
Copyright: © 2024 Tabilin et al. This is an open access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Kokaliaris C, Garba A, Matuska M, Bronzan RN, Colley DG, Dorkenoo AM, et al.. Effect of preventive chemotherapy with praziquantel on schistosomiasis among school-aged children in sub-Saharan Africa: a spatiotemporal modelling study. Lancet Infect Dis. 2022;22(1):136–49. doi: 10.1016/S1473-3099(21)00090-6 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
