

A critical role of action-related functional networks in Gilles de la Tourette syndrome
- PMID: 39681552
- PMCID: PMC11649905
- DOI: 10.1038/s41467-024-55242-6
A critical role of action-related functional networks in Gilles de la Tourette syndrome
Abstract
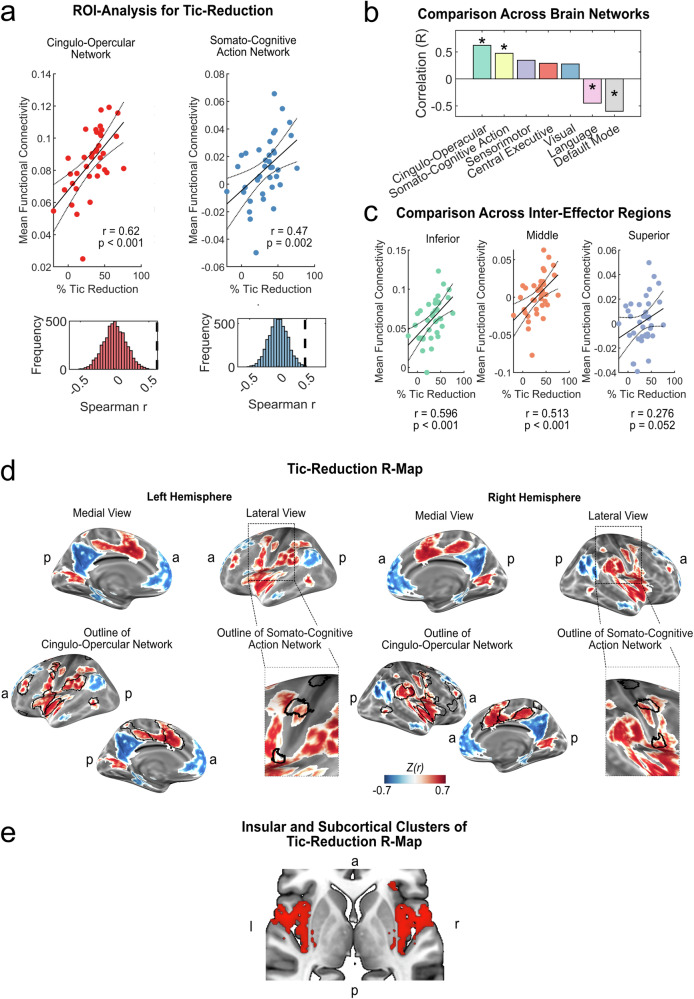
Gilles de la Tourette Syndrome (GTS) is a chronic tic disorder, characterized by unwanted motor actions and vocalizations. While brain stimulation techniques show promise in reducing tic severity, optimal target networks are not well-defined. Here, we leverage datasets from two independent deep brain stimulation (DBS) cohorts and a cohort of tic-inducing lesions to infer critical networks for treatment and occurrence of tics by mapping stimulation sites and lesions to a functional connectome derived from 1,000 healthy participants. We find that greater tic reduction is linked to higher connectivity of DBS sites (N = 37) with action-related functional resting-state networks, i.e., the cingulo-opercular (r = 0.62; p < 0.001) and somato-cognitive action networks (r = 0.47; p = 0.002). Regions of the cingulo-opercular network best match the optimal connectivity profiles of thalamic DBS. We replicate the significance of targeting cingulo-opercular and somato-cognitive action network connectivity in an independent DBS cohort (N = 10). Finally, we demonstrate that tic-inducing brain lesions (N = 22) exhibit similar connectivity to these networks. Collectively, these results suggest a critical role for these action-related networks in the pathophysiology and treatment of GTS.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: C.G. was supported by the VolkswagenStiftung (Freigeist) and received lecture honoraria from the Movement Disorder Society. K.M.V. has received financial or material research support from DFG: GZ MU 1527/3–1 GZ MU 1527/3–2, and Almirall Hermal GmbH. She has received consultants and other honoraria from Canymed, Emalex, Eurox Group, Sanity Group, Stadapharm GmbH, Swiss alpinapharm, Synendos Therapeutics AG, Tetrapharm, and Triaspharm. She is an advisory/scientific board member for Branchenverband Cannabiswirtschaft e.V. (BvCW), Sanity Group, Synendos Therapeutics AG, Syqe Medical Ltd., and Therapix Biosciences Ltd. She has received speaker’s fees from Almirall, Bundesverband der pharmazeutischen Cannabinoidunternehmen (BPC), Cogitando GmbH, Emalex, Grow, Medizinischer Dienst Westfalen Lippe, Noema, streamedup! GmbH, and Vidal. She has received royalties from Elsevier, Medizinisch Wissenschaftliche Verlagsgesellschaft Berlin, and Kohlhammer. She is an associate editor for “Cannabis and Cannabinoid Research” and an Editorial Board Member of “Medical Cannabis and Cannabinoids” und “MDPI‐Reports” and a Scientific board member for “Zeitschrift für Allgemeinmedizin”. A.H. reports lecture fees for Boston Scientific and is a consultant for FxNeuromodulation and Abbott. V.V.V. reports lecture fees for Medtronic and Boston Scientific. J.K.K. is a consultant to Boston Scientific, Medtronic, aleva and Inomed. N.S. has received financial and material research support from the research grant from the Medical University of Warsaw, the Polish Ministry of Health, the Polish Neurological Society, the Foundation for Polish Research, the European Stroke Organization, the American Academy of Neurology, American Brain Foundation and Tourette Association of America. She has received honoraria from Biogen and 90 Consulting. G.R.F. serves as an editorial board member of Cortex, Neurological Research and Practice, NeuroImage: Clinical, Zeitschrift für Neuropsychologie, and Info Neurologie & Psychiatrie; receives royalties from the publication of the books Funktionelle MRT in Psychiatrie und Neurologie, Neurologische Differentialdiagnose, SOP Neurologie, and Therapiehandbuch Neurologie; receives royalties from the publication of the neuropsychological tests KAS and Köpps; received honoraria for speaking engagements from Deutsche Gesellschaft für Neurologie (DGN) and Forum für medizinische Fortbildung FomF GmbH. All other authors report no competing interests.
Figures





References
-
- Baldermann, J. C. et al. Deep brain stimulation for Tourette-syndrome: A systematic review and meta-analysis. Brain Stimul.9, 296–304 (2016). - PubMed
-
- Conceição, V. A., Dias, Â., Farinha, A. C. & Maia, T. V. Premonitory urges and tics in Tourette syndrome: computational mechanisms and neural correlates. Curr. Opin. Neurobiol.46, 187–199 (2017). - PubMed
-
- Ganos, C., Rothwell, J. & Haggard, P. Voluntary inhibitory motor control over involuntary tic movements. Mov. Disord.33, 937–946 (2018). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
