

Interpretable multimodal machine learning (IMML) framework reveals pathological signatures of distal sensorimotor polyneuropathy
- PMID: 39681608
- PMCID: PMC11649904
- DOI: 10.1038/s43856-024-00637-1
Interpretable multimodal machine learning (IMML) framework reveals pathological signatures of distal sensorimotor polyneuropathy
Abstract
Background: Distal sensorimotor polyneuropathy (DSPN) is a common neurological disorder in elderly adults and people with obesity, prediabetes and diabetes and is associated with high morbidity and premature mortality. DSPN is a multifactorial disease and not fully understood yet.
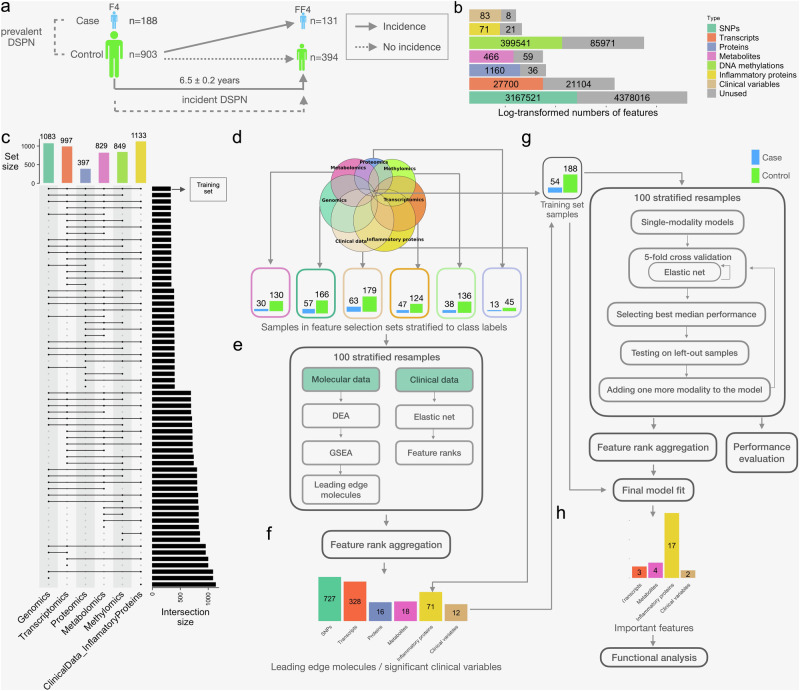
Methods: Here, we developed the Interpretable Multimodal Machine Learning (IMML) framework for predicting DSPN prevalence and incidence based on sparse multimodal data. Exploiting IMMLs interpretability further empowered biomarker identification. We leveraged the population-based KORA F4/FF4 cohort including 1091 participants and their deep multimodal characterisation, i.e. clinical data, genomics, methylomics, transcriptomics, proteomics, inflammatory proteins and metabolomics.
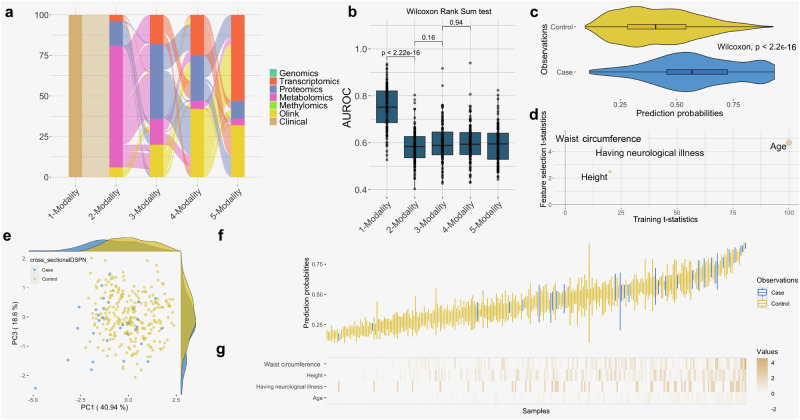
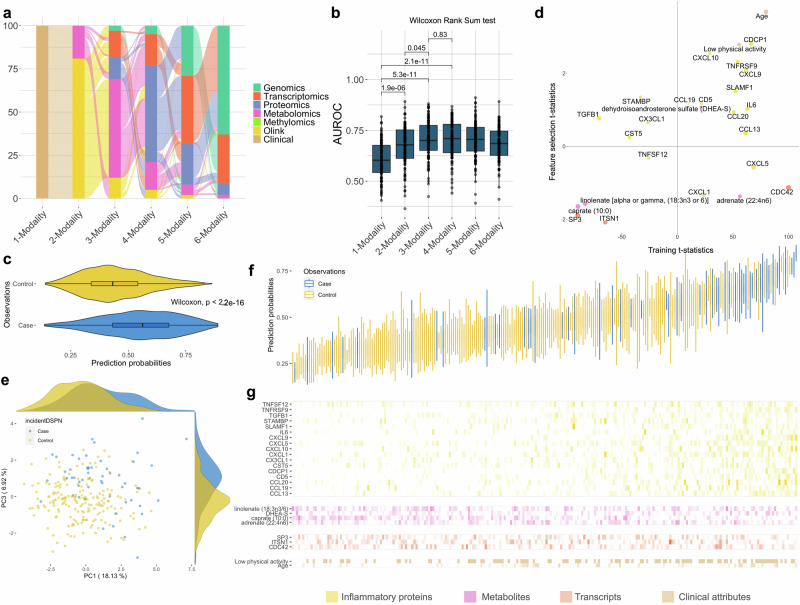
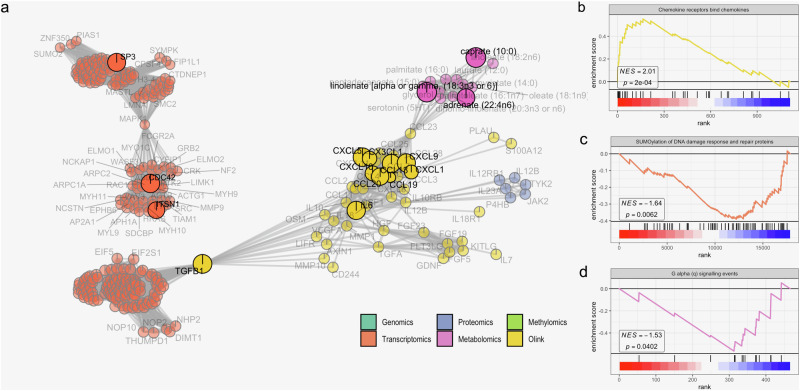
Results: Clinical data alone is sufficient to stratify individuals with and without DSPN (AUROC = 0.752), whilst predicting DSPN incidence 6.5 ± 0.2 years later strongly benefits from clinical data complemented with two or more molecular modalities (improved ΔAUROC > 0.1, achieved AUROC of 0.714). Important and interpretable features of incident DSPN prediction include up-regulation of proinflammatory cytokines, down-regulation of SUMOylation pathway and essential fatty acids, thus yielding novel insights in the disease pathophysiology.
Conclusions: These may become biomarkers for incident DSPN, guide prevention strategies and serve as proof of concept for the utility of IMML in studying complex diseases.
Plain language summary
Distal sensorimotor polyneuropathy (DSPN) is a common neurological disorder in elderly adults and people with obesity, prediabetes, and diabetes in which there is tingling or numbness with or without pain. It is not fully understood why it develops. We developed a computational method that uses various sources of information to enable people with DSPN to be identified and also to predict which people might develop DSPN in the future. Further development of our method might provide additional information that can be used to prevent development of DSPN in people with obesity, prediabetes, and diabetes. Also, our method could potentially be adapted to enable other complex diseases to be better understood.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: The authors declare no competing interests.
Figures
References
-
- Health Organization. Global Health Estimates 2016: Deaths by Cause, Age, Sex, by Country and by Region, 2000–2016. (World Health Organization, Geneva, 2018).
LinkOut - more resources
Full Text Sources
