

Patterns and drivers of excess mortality during the COVID-19 pandemic in 13 Western European countries
- PMID: 39681939
- PMCID: PMC11626765
- DOI: 10.1186/s44263-024-00103-z
Patterns and drivers of excess mortality during the COVID-19 pandemic in 13 Western European countries
Abstract
Background: Important differences in excess mortality between European countries during the COVID-19 pandemic have been reported. Understanding the drivers of these differences is essential to pandemic preparedness.
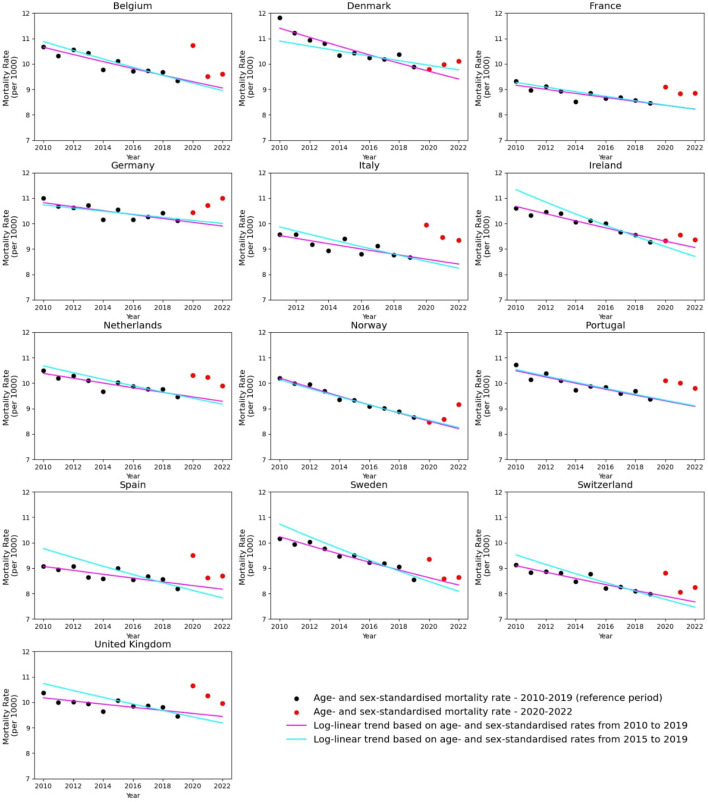
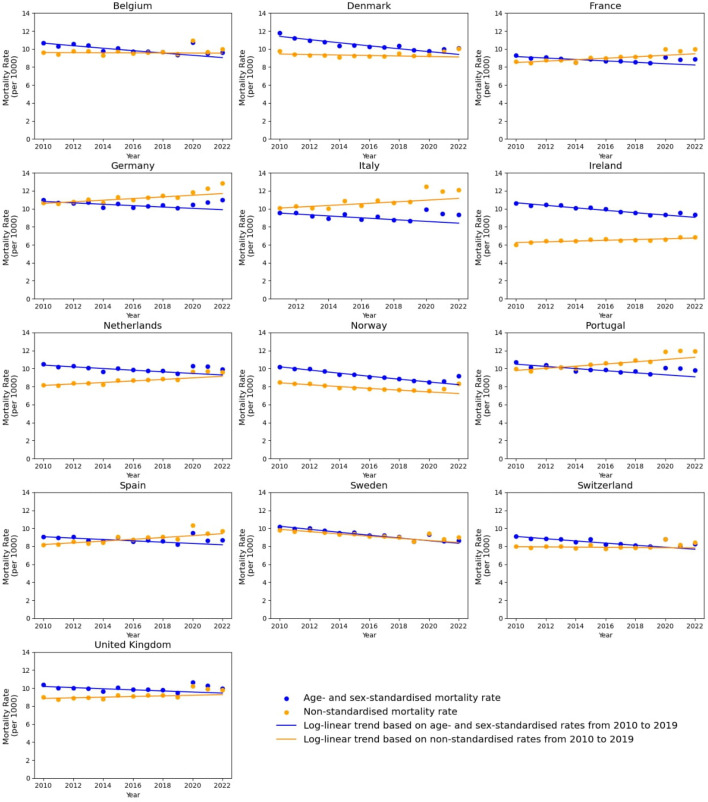
Methods: We examined patterns in age- and sex-standardized cumulative excess mortality in 13 Western European countries during the first 30 months of the COVID-19 pandemic and the correlation of country-level characteristics of interest with excess mortality.
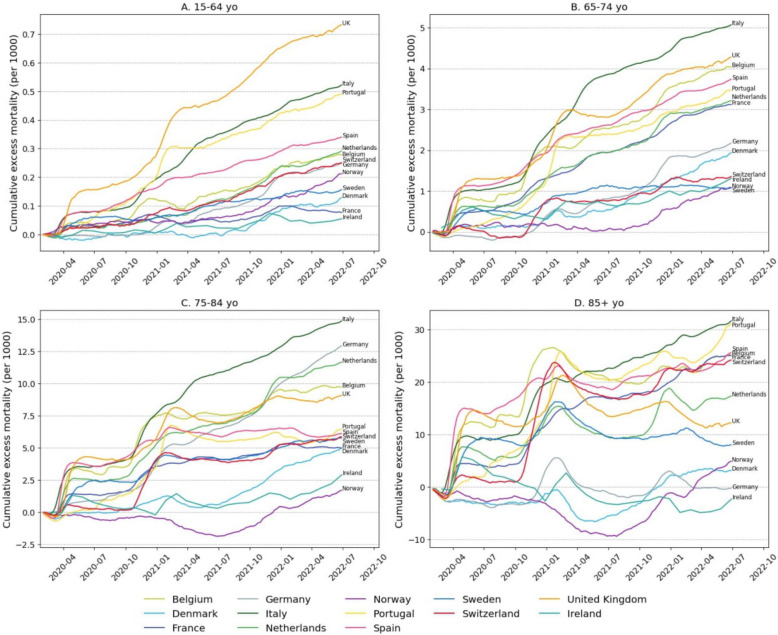
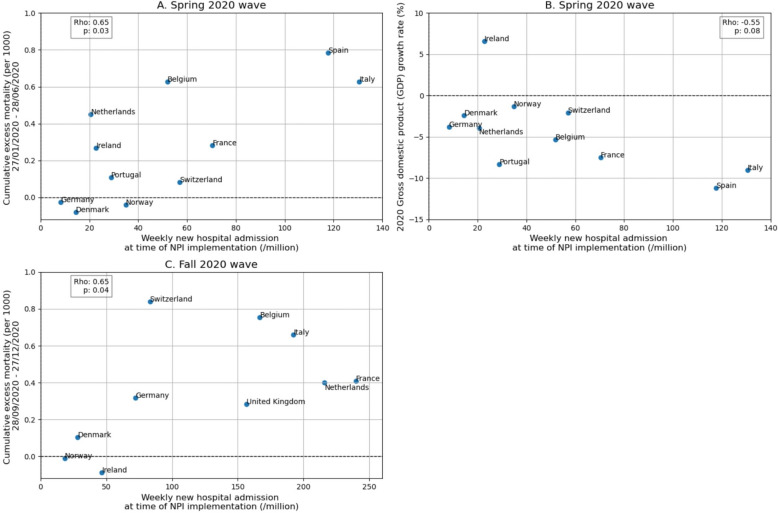
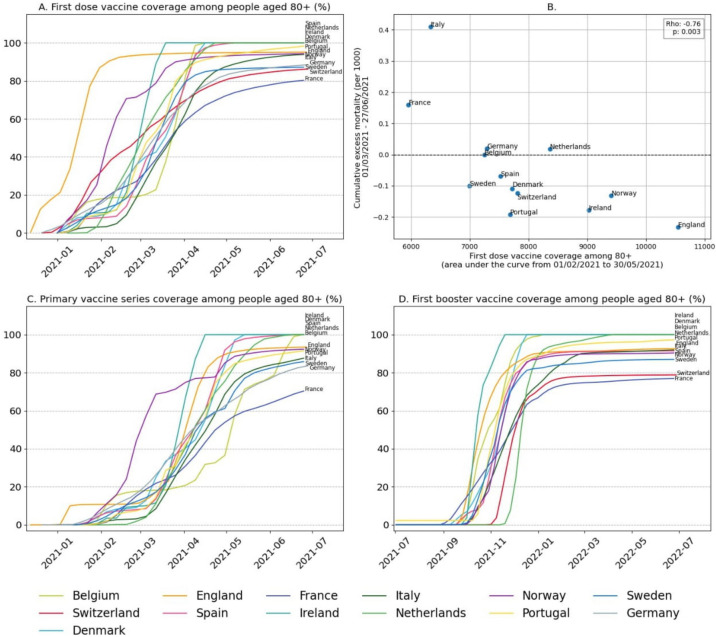
Results: In a timeline analysis, we identified notable differences in seeding events, particularly in early 2020 and when the Alpha variant emerged, likely contributing to notable differences in excess mortality between countries (lowest in Denmark during that period). These differences were more limited from July 2021 onwards. Lower excess mortality was associated with implementing stringent non-pharmaceutical interventions (NPIs) when hospital admissions were still low in 2020 (correlation coefficient rho = 0.65, p = 0.03) and rapid rollout of vaccines in the elderly in early 2021 (rho = - 0.76, p = 0.002). Countries which implemented NPIs while hospital admissions were low tended to experience lower gross domestic product (GDP) losses in 2020 (rho = - 0.55, p = 0.08). Structural factors, such as high trust in the national government (rho = - 0.77, p = 0.002) and low ratio of population at risk of poverty (rho = 0.55, p = 0.05), were also associated with lower excess mortality.
Conclusions: These results suggest the benefit of early implementation of NPIs and swift rollout of vaccines to the most vulnerable. Further analyses are required at a more granular level to better understand how these factors impacted excess mortality and help guide pandemic preparedness plans.
Keywords: COVID-19; COVID-19 / prevention & control; COVID-19 vaccines; Western Europe.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethics approval and consent to participate: Not applicable. Consent for publication: Not applicable. Competing interests: The authors declare no competing interests.
Figures

References
-
- World Health Organization. Global excess deaths associated with COVID-19 (modelled estimates) n.d. https://www.who.int/data/sets/global-excess-deaths-associated-with-covid... . Accessed 11 Apr 2024.
-
- Shalal A. IMF sees cost of COVID pandemic rising beyond $12.5 trillion estimate. Reuters. 2022.
LinkOut - more resources
Full Text Sources