

Postoperative Radiotherapy for pT1- and pT2-Classified Squamous Cell Carcinoma of the External Auditory Canal
- PMID: 39682212
- PMCID: PMC11640678
- DOI: 10.3390/cancers16234026
Postoperative Radiotherapy for pT1- and pT2-Classified Squamous Cell Carcinoma of the External Auditory Canal
Abstract
Background: There is no consensus regarding the indication for postoperative radiotherapy (PORT) for T1- and T2-classified squamous cell carcinoma (SCC) of the external auditory canal (EAC) even with negative surgical margins. This study aimed to evaluate whether PORT provides additional benefits for these cases.
Methods: We collected retrospective data from fourteen international hospitals, including resected pT1- and pT2-classified EAC SCC with negative surgical margins.
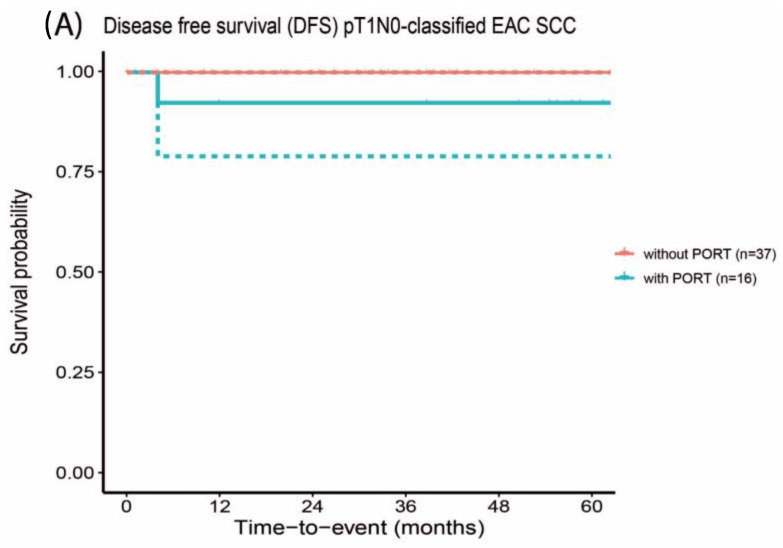
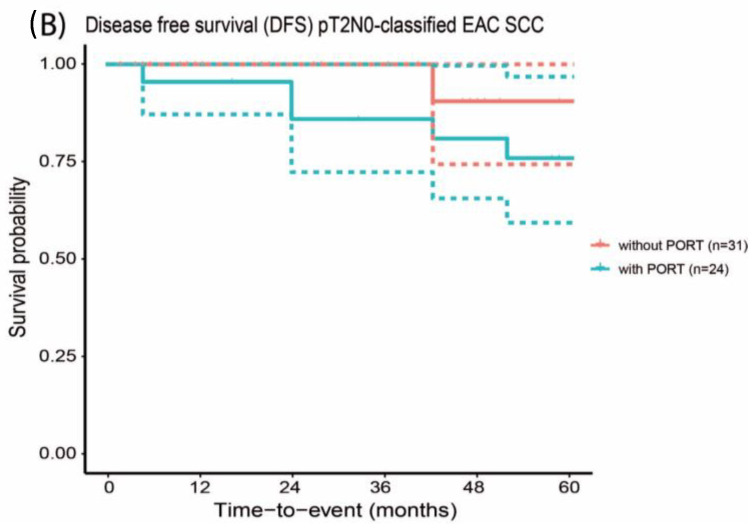
Results: A total of 112 early-stage radically resected EAC SCC were included, with 48 patients receiving PORT. The 5-year DFS of T1- and T2-classified EAC SCC treated with PORT was not statistically significantly different (92.9% and 76.9%, respectively) compared to the group treated without PORT (100% and 90.9%, respectively; p-values of 0.999 and 0.526, respectively). EAC SCC treated with PORT more frequently exhibited perineural and angioinvasive growth. Eighteen patients experienced side effects related to radiotherapy, of which one patient developed osteoradionecrosis.
Conclusions: Our study suggests that PORT for early-stage radically resected EAC SCC should only be considered in selected cases with perineural, infiltrative growth or angioinvasive growth, and with a close margin. This approach helps mitigate the negative impact on quality of life and the risk of side effects associated with radiotherapy.
Keywords: disease-free survival; radiotherapy; squamous cell carcinoma; temporal bone; treatment.
Conflict of interest statement
The authors declare that there are no conflicts of interest.
Figures
Similar articles
-
Prescription of Controlled Substances: Benefits and Risks.2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. 2025 Jul 6. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 30726003 Free Books & Documents.
-
Treatment outcomes of squamous cell carcinoma of the external auditory canal and potential benefit of induction chemotherapy followed by chemoradiotherapy.Front Oncol. 2025 Aug 15;15:1530922. doi: 10.3389/fonc.2025.1530922. eCollection 2025. Front Oncol. 2025. PMID: 40896443 Free PMC article.
-
St Andrews Referral Delay in Skin Cancer (StARDISC): a study of keratinocyte skin cancer time to treatment, growth, invasiveness, British Association of Dermatologists risk factors and excision adequacy.Br J Dermatol. 2025 Jun 20;193(1):157-166. doi: 10.1093/bjd/ljaf097. Br J Dermatol. 2025. PMID: 40080699
-
Minimally invasive surgery versus radiotherapy/chemoradiotherapy for small-volume primary oropharyngeal carcinoma.Cochrane Database Syst Rev. 2016 Dec 11;12(12):CD010963. doi: 10.1002/14651858.CD010963.pub2. Cochrane Database Syst Rev. 2016. PMID: 27943254 Free PMC article.
-
Positron emission tomography-adapted therapy for first-line treatment in individuals with Hodgkin lymphoma.Cochrane Database Syst Rev. 2015 Jan 9;1(1):CD010533. doi: 10.1002/14651858.CD010533.pub2. Cochrane Database Syst Rev. 2015. Update in: Cochrane Database Syst Rev. 2025 Mar 26;3:CD010533. doi: 10.1002/14651858.CD010533.pub3. PMID: 25572491 Free PMC article. Updated.
References
LinkOut - more resources
Full Text Sources
Research Materials
