

Limited Thyroidectomy Achieves Equivalent Survival to Total Thyroidectomy for Early Localized Medullary Thyroid Cancer
- PMID: 39682246
- PMCID: PMC11640154
- DOI: 10.3390/cancers16234062
Limited Thyroidectomy Achieves Equivalent Survival to Total Thyroidectomy for Early Localized Medullary Thyroid Cancer
Abstract
Background: The optimal surgical approach for localized T1 medullary thyroid cancer remains unclear. Total thyroidectomy is standard, but lobectomy and subtotal thyroidectomy may minimize mortality while maintaining oncologic control.
Methods: This retrospective analysis utilized the National Cancer Institute's Surveillance, Epidemiology, and End Results registry to identify 2702 MTC patients including 398 patients with T1N0/1M0 MTC treated with total thyroidectomy or lobectomy/subtotal thyroidectomy from 2000 to 2019. Cox regression analyses assessed thyroid cancer-specific and overall mortality.
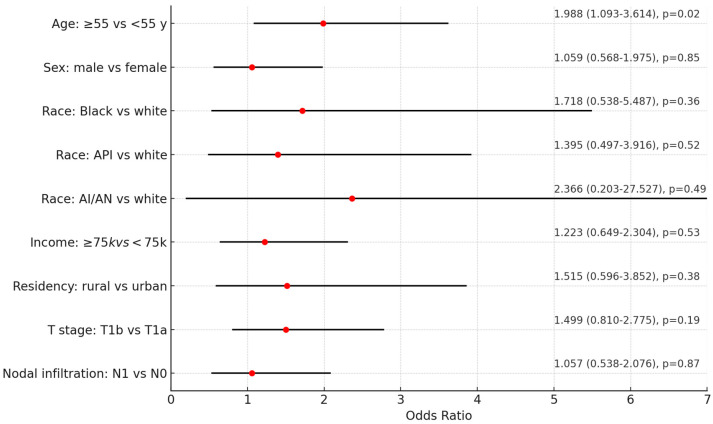
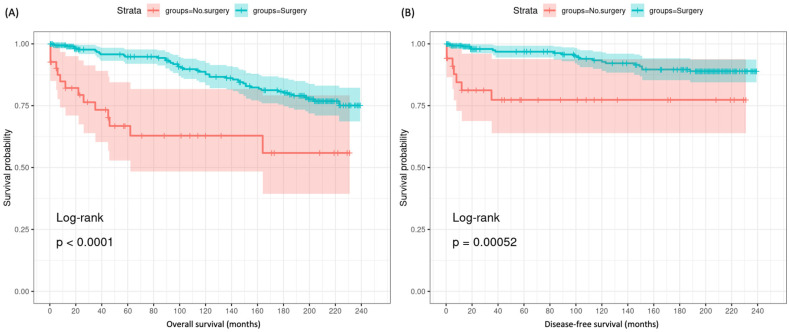
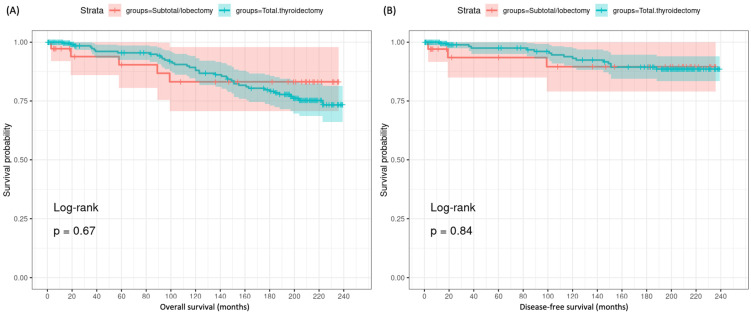
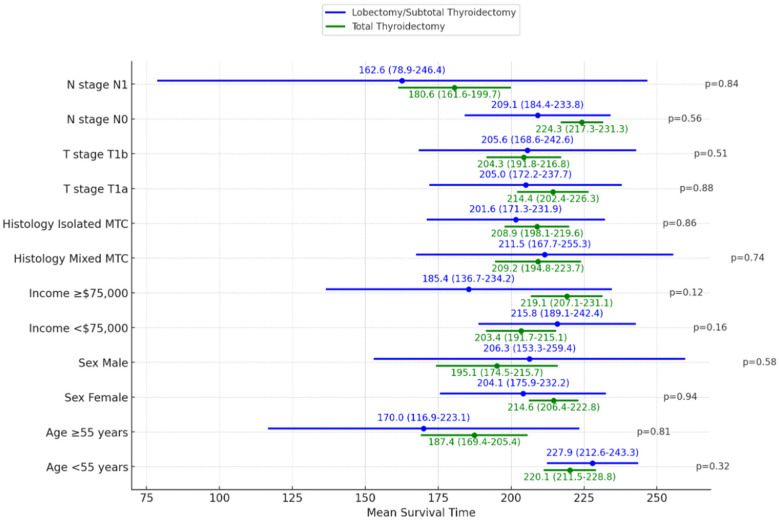
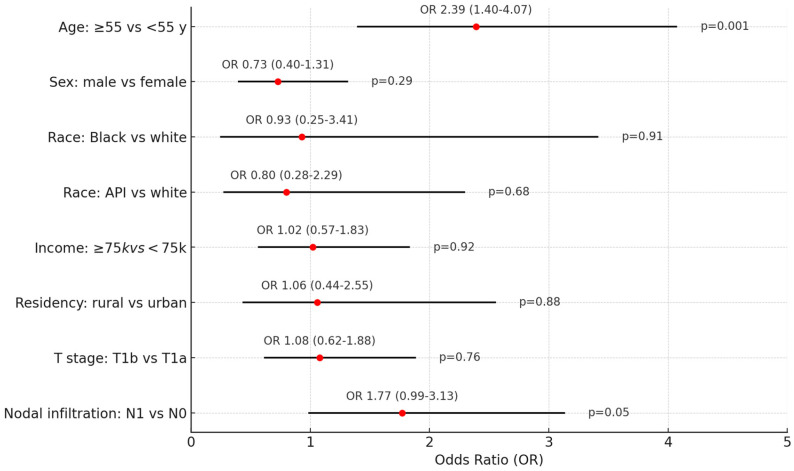
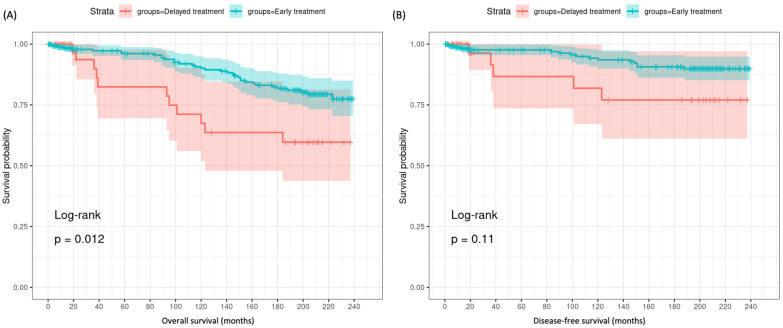
Results: The majority (89.7%) underwent total thyroidectomy, while 10.3% had lobectomy/subtotal thyroidectomy. Nodal metastases were present in 29.6%. Over a median follow-up of 8.75 years, no significant difference was observed in cancer-specific mortality (5.7% vs. 8.1%, p = 0.47) or overall mortality (13.2% vs. 12.8%, p = 0.95). On multivariate analysis, undergoing cancer-directed surgery was associated with significantly improved overall survival (HR 0.18, p < 0.001) and cancer-specific survival (HR 0.17, p < 0.001) compared to no surgery. However, no significant survival difference was seen between total thyroidectomy and lobectomy/subtotal thyroidectomy for overall mortality (HR 0.77, p = 0.60) or cancer-specific mortality (HR 0.44, p = 0.23). The extent of surgery also did not impact outcomes within subgroups stratified by age, gender, T stage, or nodal status. Delayed surgery >1 month after diagnosis was associated with worse overall survival (p = 0.012).
Conclusions: For localized T1 MTC, lobectomy/subtotal thyroidectomy appears to achieve comparable long-term survival to total thyroidectomy in this population-based analysis. The selective use of limited thyroidectomy may be reasonable for low-risk T1N0/1M0 MTC patients. Delayed surgery is associated with worse survival and additional neck dissection showed no benefit for this select group of patients.
Keywords: MTC; SEER; T1N0M0; T1N1M0; endocrine; lobectomy; medullary thyroid cancer; thyroidectomy.
Conflict of interest statement
The authors declare no conflicts of interest. The research was presented in the Annual Meeting of the American Thyroid Association, Chicago, IL, 1 November 2024.
Figures
Similar articles
-
Total thyroidectomy vs thyroid lobectomy for localized medullary thyroid cancer in adults: A propensity-matched survival analysis.Surgery. 2022 Nov;172(5):1385-1391. doi: 10.1016/j.surg.2022.06.023. Epub 2022 Aug 20. Surgery. 2022. PMID: 35995619
-
Lobectomy may be more appropriate for patients with early-stage medullary thyroid cancer older than 60 years old.Front Endocrinol (Lausanne). 2022 Oct 21;13:1015319. doi: 10.3389/fendo.2022.1015319. eCollection 2022. Front Endocrinol (Lausanne). 2022. PMID: 36339396 Free PMC article.
-
Medullary thyroid carcinoma: clinical characteristics, treatment, prognostic factors, and a comparison of staging systems.Cancer. 2000 Mar 1;88(5):1139-48. doi: 10.1002/(sici)1097-0142(20000301)88:5<1139::aid-cncr26>3.0.co;2-z. Cancer. 2000. PMID: 10699905
-
An Overview of Medullary Thyroid Cancer Cases Treated at Kuwait Cancer Control Center.Gulf J Oncolog. 2020 Sep;1(34):39-47. Gulf J Oncolog. 2020. PMID: 33431361 Review.
-
Long-Term Follow-up in Medullary Thyroid Carcinoma.Recent Results Cancer Res. 2015;204:207-25. doi: 10.1007/978-3-319-22542-5_10. Recent Results Cancer Res. 2015. PMID: 26494391 Review.
References
LinkOut - more resources
Full Text Sources
