

Molecular Composition and Kinetics of B Cells During Ibrutinib Treatment in Patients with Chronic Lymphocytic Leukemia
- PMID: 39684282
- PMCID: PMC11641073
- DOI: 10.3390/ijms252312569
Molecular Composition and Kinetics of B Cells During Ibrutinib Treatment in Patients with Chronic Lymphocytic Leukemia
Abstract
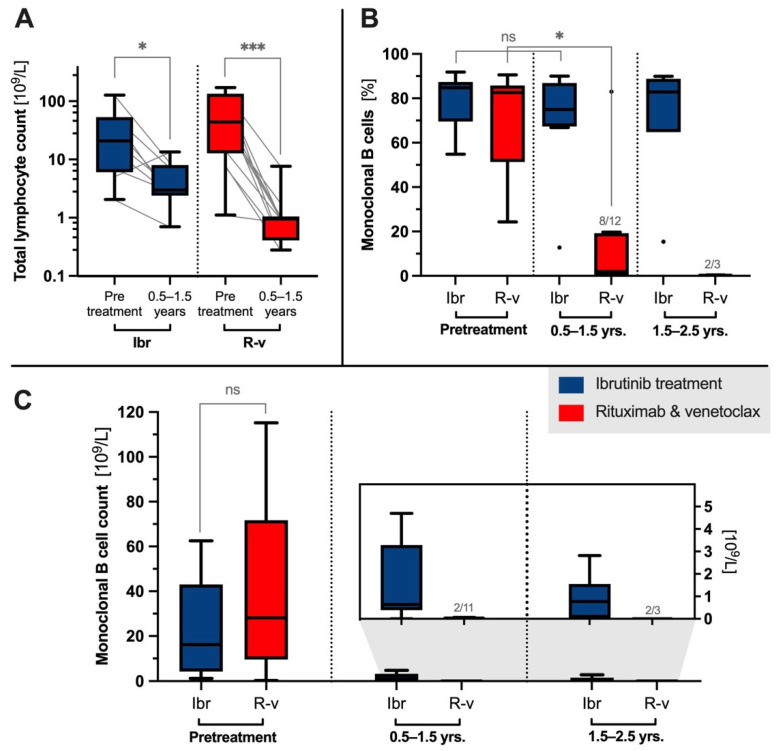
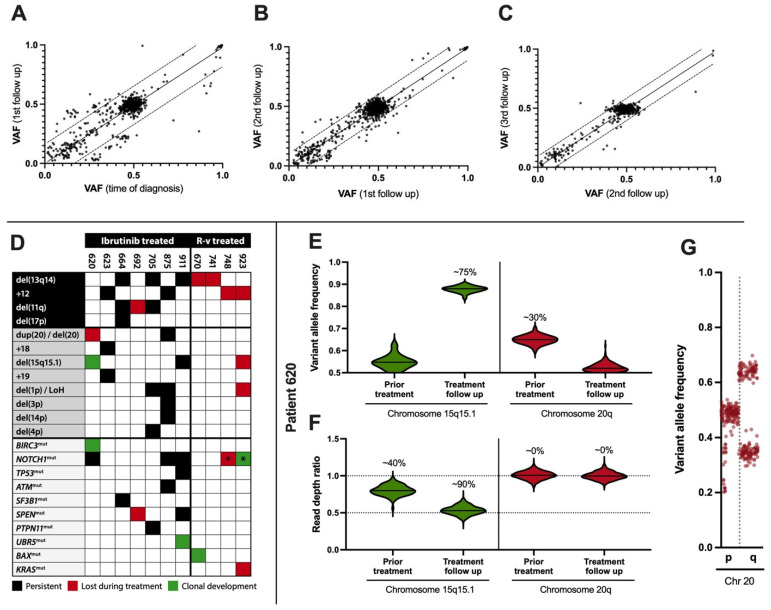
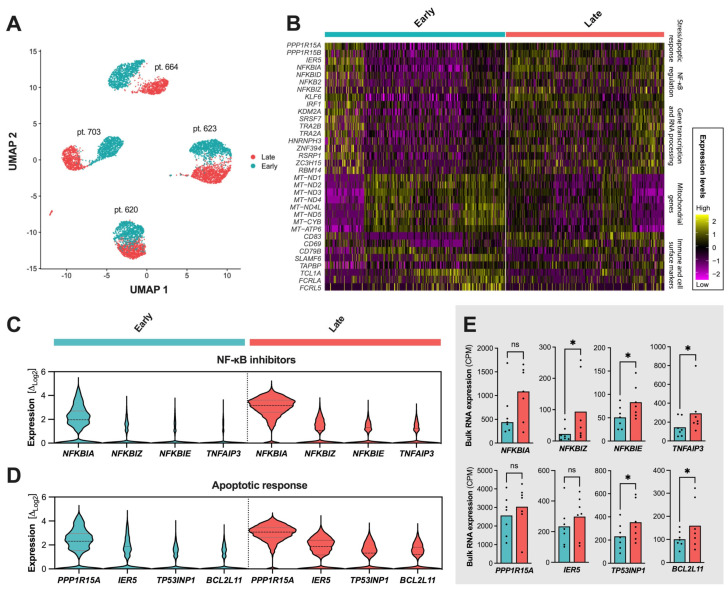
Chronic lymphocytic leukemia (CLL) is characterized by the accumulation of B cells due to constitutive B-cell receptor (BCR) signaling, leading to apoptosis resistance and increased proliferation. This study evaluates the effects of the Bruton Tyrosine Kinase (BTK) inhibitor ibrutinib on the molecular composition, clonality, and kinetics of B cells during treatment in CLL patients. Employing a multi-omics approach of up to 3.2 years of follow-up, we analyzed data from 24 CLL patients, specifically focusing on nine patients treated with ibrutinib monotherapy. In this study, clonal stability was observed within the ibrutinib-treated group following an effective initial clinical response, where clonotype frequencies of residual CLL cells remained high and stable, ranging from 74.9% at 1.5 years to 87.7% at approximately 3 years. In contrast, patients treated with the B-cell lymphoma 2 (BCL2) inhibitor venetoclax exhibited substantial reductions in clonal frequencies, approaching molecular eradication. Deep whole-exome sequencing revealed minimal genomic progression in the ibrutinib group, maintaining somatic drivers and variant allele frequencies (VAF) above 0.2 throughout treatment. At the single-cell level, the NF-κB pathway inhibition and apoptotic signals were detected or even augmented during treatment in ibrutinib-treated patients. These findings may corroborate the role of ibrutinib in stabilizing the genomic landscape of CLL cells, preventing significant genomic evolution despite maintaining a high clonal burden within the residual B-cell compartment.
Keywords: chronic lymphocytic leukemia; clonal stability; ibrutinib; lymphocytosis; molecular profiling; treatment efficacy.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- de Rooij M.F., Kuil A., Geest C.R., Eldering E., Chang B.Y., Buggy J.J., Pals S.T., Spaargaren M. The clinically active BTK inhibitor PCI-32765 targets B-cell receptor- and chemokine-controlled adhesion and migration in chronic lymphocytic leukemia. Blood. 2012;119:2590–2594. doi: 10.1182/blood-2011-11-390989. - DOI - PubMed
-
- Herman S.E., Gordon A.L., Hertlein E., Ramanunni A., Zhang X., Jaglowski S., Flynn J., Jones J., Blum K.A., Buggy J.J., et al. Bruton tyrosine kinase represents a promising therapeutic target for treatment of chronic lymphocytic leukemia and is effectively targeted by PCI-32765. Blood. 2011;117:6287–6296. doi: 10.1182/blood-2011-01-328484. - DOI - PMC - PubMed
-
- Ponader S., Chen S.S., Buggy J.J., Balakrishnan K., Gandhi V., Wierda W.G., Keating M.J., O’Brien S., Chiorazzi N., Burger J.A. The Bruton tyrosine kinase inhibitor PCI-32765 thwarts chronic lymphocytic leukemia cell survival and tissue homing in vitro and in vivo. Blood. 2012;119:1182–1189. doi: 10.1182/blood-2011-10-386417. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
- R246-A14603/Danish Cancer Society
- R281-16686/Danish Cancer Society
- 60988/Helen Rudes Fund
- R90-A4022/OUH PhD Fund
- NA/Dagmar Marshalls Fund
- 2304/Agnes og Poul Friis Fund, Tornøe's og Høyrup's Fund
- NA/Marie og Børge Kroghs Fund
- NA/Torben og Alice Frimodts Fund
- NA/Danish Lymphoma Group Grant
- 5523-TL-ne/Grosserer M. Brogaard og hustrus Mindefond Odense
- NA/Folketingsmand J. Christensen og hustru K. Christensens Fund
- A37628/Brødrene Hartmanns Fund
LinkOut - more resources
Full Text Sources
