

Diagnostic Accuracy of Dynamic High-Resolution Ultrasonography in Assessing Anterior Disc Displacement in Temporomandibular Joint Disorders: A Prospective Observational Study
- PMID: 39684977
- PMCID: PMC11641683
- DOI: 10.3390/healthcare12232355
Diagnostic Accuracy of Dynamic High-Resolution Ultrasonography in Assessing Anterior Disc Displacement in Temporomandibular Joint Disorders: A Prospective Observational Study
Abstract
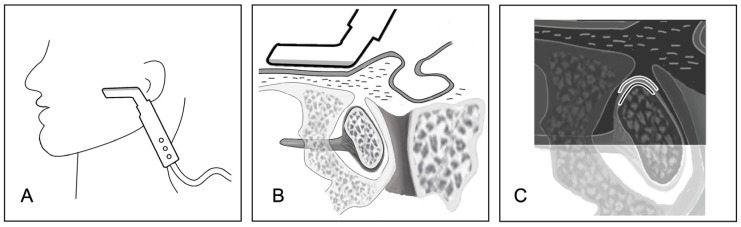
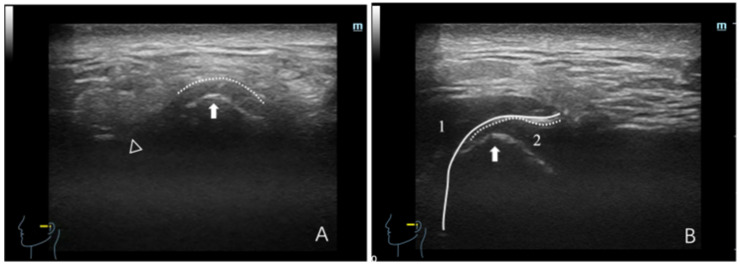
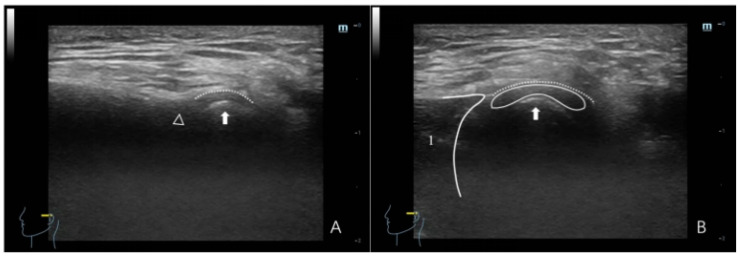
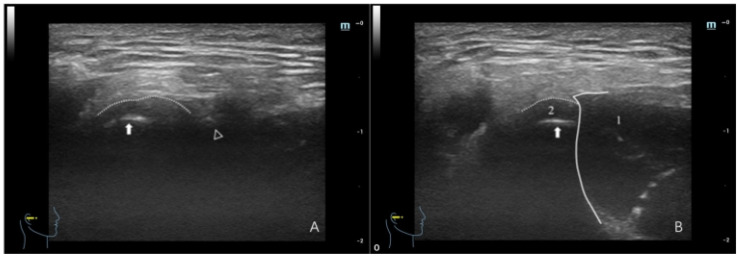
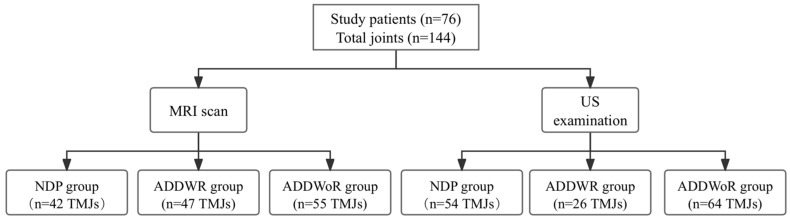
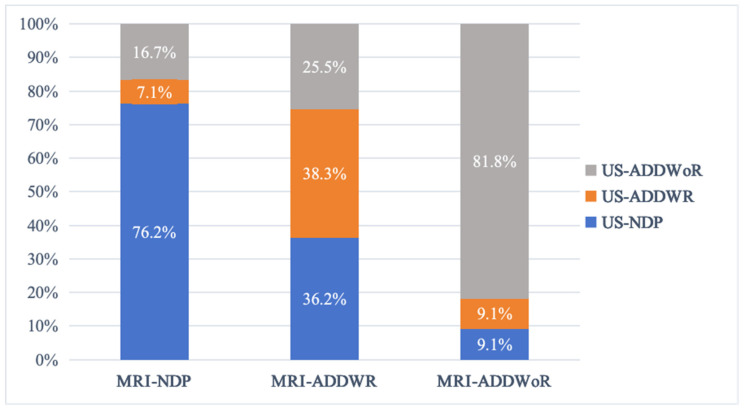
Objective: The objective of this study was to assess the diagnostic efficacy of dynamic high-resolution ultrasonography (HRUS) in detecting anterior disc displacement with reduction (ADDWR) and anterior disc displacement without reduction (ADDWoR) in the temporomandibular joint (TMJ). Methods: A total of 144 TMJs was categorized into three groups according to the magnetic resonance imaging (MRI) findings, which served as the reference standard: the normal disc position (NDP) group, the ADDWR group, and the ADDWoR group. Static images of the TMJ in full opening and maximum intercuspal positions, along with dynamic sequences during jaw opening, were obtained utilizing a 14 MHz L-shaped linear array transducer. The diagnostic efficacy of dynamic HRUS for identifying ADDWR and ADDWoR was evaluated in terms of accuracy, sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), diagnostic odds ratio (DOR), and the Youden index. Results: According to the MRI findings, the NDP, ADDWR, and ADDWoR groups consisted of 42 (29.2%), 47 (32.6%), and 55 (38.2%) TMJs, respectively. HRUS data revealed 54 TMJs (37.5%) in the NDP group, 26 TMJs (18.1%) in the ADDWR group, and 64 TMJs (44.4%) in the ADDWoR group. With MRI as the reference standard, HRUS exhibited a diagnostic accuracy of 71.4%, sensitivity of 51.4%, and specificity of 91.4% for ADDWR. For the ADDWoR, HRUS attained a diagnostic accuracy of 86.5%, sensitivity of 90.0%, and specificity of 82.1%. Conclusions: With MRI serving as the reference standard, dynamic HRUS has high diagnostic value for ADDWoR, with better diagnostic accuracy than ADDWR. Ultrasonography has the potential to be used as a highly effective and non-invasive imaging modality for the early screening of ADD in future clinical practice.
Keywords: anterior disc displacement; diagnostic efficacy; dynamic high-resolution ultrasonography; temporomandibular joint disorders.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
[A three-dimensional imaging study of the effect of anterior disc displacement on the bony structural relationship of the temporomandibular joint].Zhonghua Kou Qiang Yi Xue Za Zhi. 2024 Feb 9;59(2):157-164. doi: 10.3760/cma.j.cn112144-20230718-00015. Zhonghua Kou Qiang Yi Xue Za Zhi. 2024. PMID: 38280823 Chinese.
-
[The diagnostic value of high-resolution ultrasonography for detecting anterior disc displacement without reduction of temporomandibular joint].Hua Xi Kou Qiang Yi Xue Za Zhi. 2012 Dec;30(6):632-4, 640. Hua Xi Kou Qiang Yi Xue Za Zhi. 2012. PMID: 23330376 Chinese.
-
Role of Dynamic 3 Tesla MRI in the Evaluation of Temporomandibular Joint Dysfunction.Cureus. 2023 Mar 25;15(3):e36681. doi: 10.7759/cureus.36681. eCollection 2023 Mar. Cureus. 2023. PMID: 37113366 Free PMC article.
-
Evaluation of clinical signs and magnetic resonance imaging findings in patients with temporomandibular disorders.J Craniomaxillofac Surg. 2023 Jul-Aug;51(7-8):441-447. doi: 10.1016/j.jcms.2023.08.013. Epub 2023 Aug 16. J Craniomaxillofac Surg. 2023. PMID: 37604767
-
Comparison of altered signal intensity, position, and morphology of the TMJ disc in MR images corrected for variations in surface coil sensitivity.Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006 Apr;101(4):515-22. doi: 10.1016/j.tripleo.2005.04.004. Epub 2005 Sep 19. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006. PMID: 16545717
Cited by
-
Recent advances and educational strategies in diagnostic imaging for temporomandibular disorders: a narrative literature review.Front Neurol. 2025 May 26;16:1597312. doi: 10.3389/fneur.2025.1597312. eCollection 2025. Front Neurol. 2025. PMID: 40492175 Free PMC article. Review.
References
-
- Lavinsky D., Lavinsky J., Setogutti E.T., Rehm D.D.S., Lavinsky L. The Role of Magnetic Resonance Imaging of the Temporomandibular Joint to Investigate Tinnitus in Adults with Temporomandibular Joint Disorder: A Comparative Study. Int. Arch. Otorhinolaryngol. 2020;24:e68–e72. doi: 10.1055/s-0039-1688840. - DOI - PMC - PubMed
-
- Schiffman E., Ohrbach R., Truelove E., Look J., Anderson G., Goulet J.-P., List T., Svensson P., Gonzalez Y., Lobbezoo F., et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network and Orofacial Pain Special Interest Group. J. Oral Facial Pain Headache. 2014;28:6–27. doi: 10.11607/jop.1151. - DOI - PMC - PubMed
-
- Gauer R.L., Semidey M.J. Diagnosis and Treatment of Temporomandibular Disorders. Am. Fam. Physician. 2015;91:378–386. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
