

The Impact of the Coronary Artery Calcium Score on the Clinical Outcomes in Patients with Acute Myocardial Infarction
- PMID: 39685595
- PMCID: PMC11642475
- DOI: 10.3390/jcm13237136
The Impact of the Coronary Artery Calcium Score on the Clinical Outcomes in Patients with Acute Myocardial Infarction
Abstract
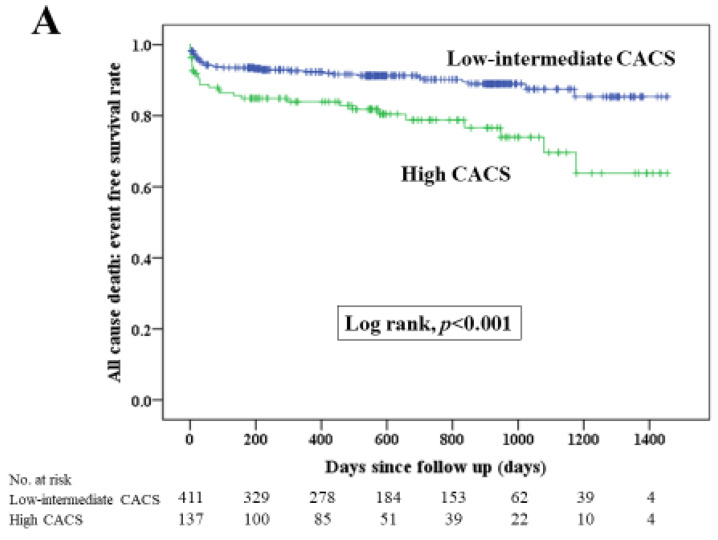
Background: It is essential to identify the risk factors for poor clinical outcomes in patients with acute myocardial infarction (AMI). The coronary artery calcium score (CACS) is gathering attention as a predictor for future cardiovascular events. This study aimed to (1) measure CACSs in patients with AMI by non-ECG-gated computed tomography (CT), (2) compare clinical outcomes between patients with a high CACS and a low-intermediate CACS and (3) to elucidate the association between high CACS and clinical outcomes. Methods: We defined the high CACS group as the highest quantile of CACS (Q4) and defined the low-intermediate CACS group as the other quantiles of CACS (Q1-Q3). The primary endpoint was major adverse cardiovascular events (MACE), which were defined as the composite of all-cause death, re-admission for heart failure, non-fatal MI and target vessel revascularization. We included 548 patients with AMI who underwent non-ECG-gated CT and divided them into the high CACS group (CACS ≥ 5346.5, n = 137) and the low-intermediate CACS group (CACS ≤ 5329.3, n = 411). Results: During the median follow-up duration of 535 days, 150 MACE were observed. The Kaplan-Meier curves showed that MACE occurred more frequently in the high CACS group than in the low-intermediate CACS group (p < 0.001). Multivariable Cox hazard analysis revealed that a high CACS was significantly associated with MACE (hazard ratio 1.597, 95% confidence interval 1.081-2.358, p = 0.019) after controlling for multiple confounding factors. Conclusions: Clinical outcomes were worse in AMI patients with a high CACS than in those with a low-intermediate CACS. A high CACS was significantly associated with MACE in multivariate analysis.
Keywords: acute myocardial infarction; coronary artery calcium score; major adverse cardiovascular events.
Conflict of interest statement
K. Sakakura received a speaking honorarium from Canon. The authors declare no conflict of interest.
Figures




References
-
- Thrane P.G., Olesen K.K.W., Thim T., Gyldenkerne C., Hansen M.K., Stodkilde-Jorgensen N., Jakobsen L., Bodtker Mortensen M., Dalby Kristensen S., Maeng M. 10-Year Mortality After ST-Segment Elevation Myocardial Infarction Compared to the General Population. J. Am. Coll. Cardiol. 2024;83:2615–2625. doi: 10.1016/j.jacc.2024.04.025. - DOI - PubMed
-
- Fox D.K., Waken R.J., Wang F., Wolfe J.D., Robbins K., Fanous E., Vader J.M., Schilling J.D., Joynt Maddox K.E. The Association of the UNOS Heart Allocation Policy Change With Transplant and Left Ventricular Assist Device Access and Outcomes. Am. J. Cardiol. 2023;204:392–400. doi: 10.1016/j.amjcard.2023.07.090. - DOI - PMC - PubMed
-
- Pedersen F., Butrymovich V., Kelbaek H., Wachtell K., Helqvist S., Kastrup J., Holmvang L., Clemmensen P., Engstrom T., Grande P., et al. Short- and long-term cause of death in patients treated with primary PCI for STEMI. J. Am. Coll. Cardiol. 2014;64:2101–2108. doi: 10.1016/j.jacc.2014.08.037. - DOI - PubMed
-
- Klein F., Crooijmans C., Peters E.J., van t‘ Veer M., Timmermans M.J.C., Henriques J.P.S., Verouden N.J.W., Kraaijeveld A.O., Bunge J.J.H., Lipsic E., et al. Impact of symptom duration and mechanical circulatory support on prognosis in cardiogenic shock complicating acute myocardial infarction. Neth. Heart J. 2024;32:290–297. doi: 10.1007/s12471-024-01881-9. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
