

COVID-19 and Cardiac Arrhythmias: Lesson Learned and Dilemmas
- PMID: 39685718
- PMCID: PMC11642268
- DOI: 10.3390/jcm13237259
COVID-19 and Cardiac Arrhythmias: Lesson Learned and Dilemmas
Abstract
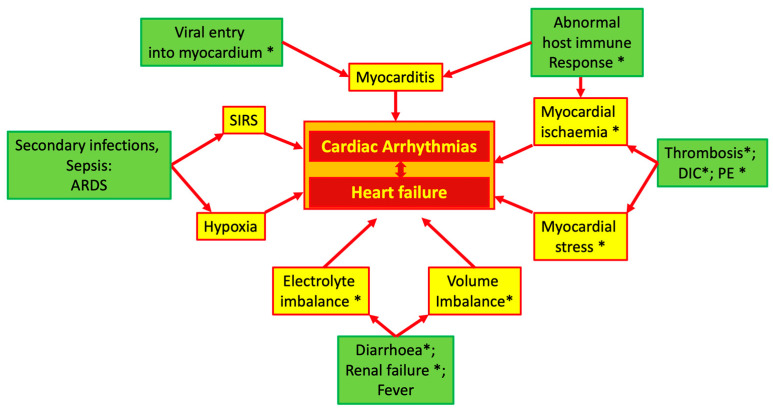
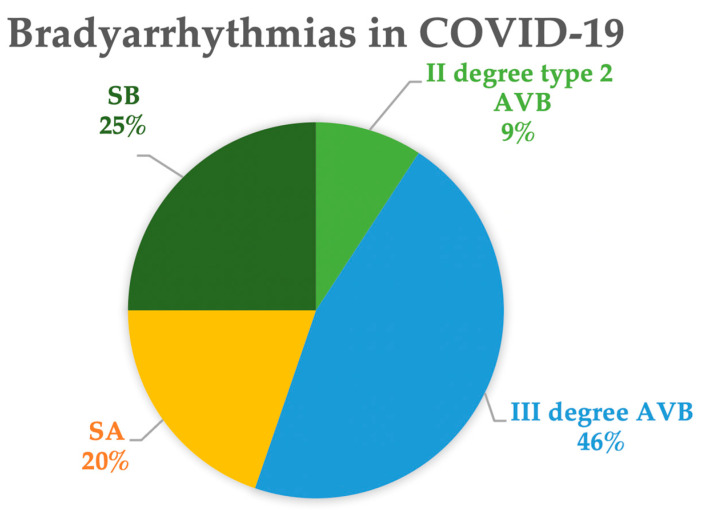
Over the last few years, COVID-19 has attracted medical attention both in terms of healthcare system reorganization and research. Among the different cardiovascular complications of the SARS-CoV-2 infection, cardiac arrhythmias represent an important clinical manifestation requiring proper therapy both in the acute and post-acute phase. The multiparametric in-hospital monitoring of COVID-19 patients frequently detects new-onset or recurrent cardiac arrhythmias. As many patients are monitored remotely from cardiology departments, this setting calls for proper arrhythmia interpretation and management, especially in critically ill patients in the intensive care unit. From this perspective, the possible pathophysiologic mechanisms and the main clinical manifestations of brady- and tachyarrhythmias in COVID-19 patients are briefly presented. The progressively increasing body of evidence on pathophysiology helps to identify the reversible causes of arrhythmias, better clarify the setting in which they occur, and establish their impact on prognosis, which are of paramount importance to orient decision making. Despite the accumulating knowledge on this disease, some dilemmas in the management of these patients may remain, such as the need to implant in the acute or post-acute phase a permanent pacemaker or cardioverter/defibrillation in patients presenting with brady- or tachyarrhythmias and lifelong oral anticoagulation in new-onset atrial fibrillation detected during SARS-CoV-2 infection.
Keywords: COVID-19; SARS-CoV-2 infection; bradyarrhythmia; cardiac arrhythmias; oral anticoagulation; tachyarrhythmias.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Similar articles
-
Arrhythmias in the intensive care patient.Curr Opin Crit Care. 2003 Oct;9(5):345-55. doi: 10.1097/00075198-200310000-00003. Curr Opin Crit Care. 2003. PMID: 14508146 Review.
-
Cardiac arrhythmias in critically ill patients with coronavirus disease 2019: A retrospective population-based cohort study.Acta Anaesthesiol Scand. 2021 Jul;65(6):770-777. doi: 10.1111/aas.13806. Epub 2021 Mar 13. Acta Anaesthesiol Scand. 2021. PMID: 33638870 Free PMC article.
-
Complications of new-onset atrial fibrillation in critically ill COVID-19 patients admitted to the intensive care unit (ICU): a meta-analysis.BMC Cardiovasc Disord. 2024 Aug 5;24(1):407. doi: 10.1186/s12872-024-04086-5. BMC Cardiovasc Disord. 2024. PMID: 39103764 Free PMC article.
-
Fatal arrhythmia associated with novel coronavirus 2019 infection: Case report and literature review.Medicine (Baltimore). 2024 Apr 19;103(16):e37894. doi: 10.1097/MD.0000000000037894. Medicine (Baltimore). 2024. PMID: 38640277 Free PMC article. Review.
-
Cardiac arrhythmias in patients with COVID-19: Lessons from 2300 telemetric monitoring days on the intensive care unit.J Electrocardiol. 2021 May-Jun;66:102-107. doi: 10.1016/j.jelectrocard.2021.04.001. Epub 2021 Apr 16. J Electrocardiol. 2021. PMID: 33906056 Free PMC article.
References
-
- Wang D., Hu B., Hu C., Zhu F., Liu X., Zhang J., Wang B., Xiang H., Cheng Z., Xiong Y., et al. Clinical Characteristics of 138 Hospitalized Patients with 2019 Novel Coronavirus-Infected Pneumonia in Wuhan, China. JAMA. 2020;323:1061–1069. doi: 10.1001/jama.2020.1585. Erratum in JAMA 2021, 325, 1113. - DOI - PMC - PubMed
-
- Gopinathannair R., Merchant F.M., Lakkireddy D.R., Etheridge S.P., Feigofsky S., Han J.K., Kabra R., Natale A., Poe S., Saha S.A., et al. COVID-19 and cardiac arrhythmias: A global perspective on arrhythmia characteristics and management strategies. J. Interv. Card. Electrophysiol. 2020;59:329–336. doi: 10.1007/s10840-020-00789-9. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
