

Is the Anamnesis Enough to De-Label Patients with Reported Beta-Lactam Allergy?
- PMID: 39685725
- PMCID: PMC11642921
- DOI: 10.3390/jcm13237267
Is the Anamnesis Enough to De-Label Patients with Reported Beta-Lactam Allergy?
Abstract
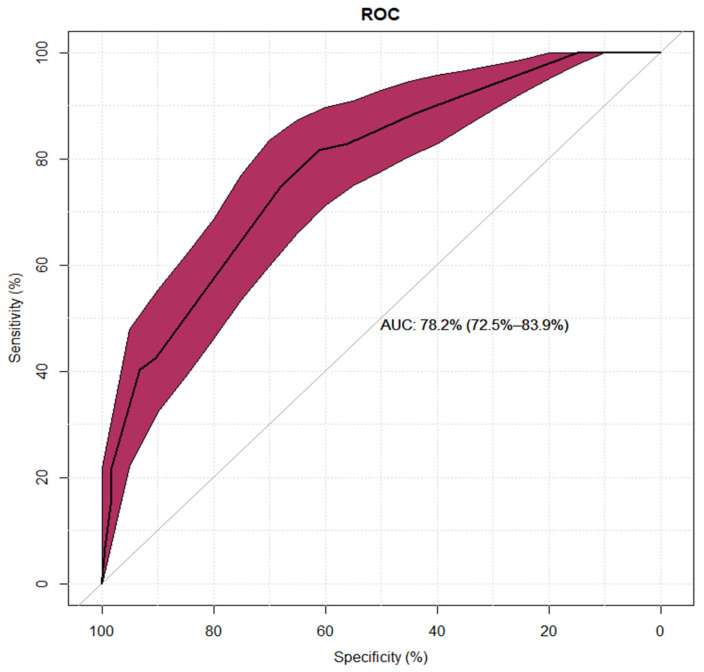
Background: The decision whether to de-label patient with suspected BL hypersensitivity is based on risk stratification. The aim of this study was to prepare a characteristic of diagnostic risk groups and to create a model enabling the identification of the low-risk diagnostic group. Methods: We analyzed the medical records of patients hospitalized due to suspected hypersensitivity to BL antibiotics. Based on their medical-history data, patients were divided into three diagnostic risk groups, using the criteria proposed by Shenoy et al. Univariate and multivariate analysis models were used to create a diagnostic tool. Results: Among 263 patients referred for BL hypersensitivity diagnosis, 88 (33.5%) were allocated to group I, 129 (49%) to group II, and 46 (17.5%) to group III. There were significant differences between diagnostic risk groups regarding history of hypersensitivity to penicillins (p < 0.001), cephalosporins (p < 0.001), >1 BL (p < 0.05), several episodes of BL hypersensitivity (p < 0.001), medical intervention (p < 0.001), documented hypersensitivity (p < 0.001), time from drug intake to symptoms (p < 0.001), and time from hypersensitivity to diagnosis (p < 0.001). In total, 81 patients (30.8%) were de-labeled: 52 (59.8%) in group I, 27 (20.9%) in group II, and 2 (4.3%) in group III. The univariate analysis model of the low-diagnostic-risk group applied to the de-labeled part showed 90% specificity and 21.93% sensitivity. NPV and PPV were estimated at 72.04% and 49.53%, respectively. The multivariate model had high specificity but low sensitivity; its NPV was 76%, with 68% PPV. Conclusions: The tool enabling the identification of low-diagnostic-risk patients based on anamnesis is not sensitive enough to de-label patients on its basis.
Keywords: beta-lactam; de-labeling; hypersensitivity; risk stratification.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
Similar articles
-
Can Beta-Lactam Allergy De-Labeling Strategies Safely Empower Geriatric Care?J Clin Med. 2025 May 15;14(10):3476. doi: 10.3390/jcm14103476. J Clin Med. 2025. PMID: 40429471 Free PMC article.
-
Adding a second skin prick test reading and modifying the cut-off for beta-lactam-specific IgE enhances the sensitivity in the routine diagnostic workup for immediate beta-lactam hypersensitivity.Contact Dermatitis. 2020 Nov;83(5):361-371. doi: 10.1111/cod.13622. Epub 2020 Jul 27. Contact Dermatitis. 2020. PMID: 32462721
-
Identifying Low-Risk Beta-Lactam Allergy Patients in a UK Tertiary Centre.J Allergy Clin Immunol Pract. 2019 Sep-Oct;7(7):2173-2181.e1. doi: 10.1016/j.jaip.2019.03.015. Epub 2019 Mar 25. J Allergy Clin Immunol Pract. 2019. PMID: 30922992
-
New diagnostıc perspectives in the management of pediatrıc beta-lactam allergy.Pediatr Allergy Immunol. 2022 Mar;33(3):e13745. doi: 10.1111/pai.13745. Pediatr Allergy Immunol. 2022. PMID: 35338725 Review.
-
Controversies in Drug Allergy: Beta-Lactam Hypersensitivity Testing.J Allergy Clin Immunol Pract. 2019 Jan;7(1):40-45. doi: 10.1016/j.jaip.2018.07.051. Epub 2018 Sep 20. J Allergy Clin Immunol Pract. 2019. PMID: 30245291 Review.
References
-
- Doña I., Caubet J.C., Brockow K., Doyle M., Moreno E., Terreehorst I., Torres M.J. An EAACI task force report: Recognising the potential of the primary care physician in the diagnosis and management of drug hypersensitivity. Clin. Transl. Allergy. 2018;8:16. doi: 10.1186/s13601-018-0202-2. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
