

Switching from natalizumab to antiCD20 monoclonal antibodies: Short transition interval is associated with improved outcome
- PMID: 39686558
- PMCID: PMC11649819
- DOI: 10.1111/ene.16587
Switching from natalizumab to antiCD20 monoclonal antibodies: Short transition interval is associated with improved outcome
Abstract
Objective: To investigate the impact of transition interval length when switching from natalizumab (NTZ) to anti-CD20 monoclonal antibodies (antiCD20) on recurrent disease activity and safety in relapsing multiple sclerosis (RMS).
Methods: Aggregating data from 8 MS centres in Austria, Switzerland, and Germany, we included RMS patients who (i) continuously received NTZ for ≥3 months, (ii) were switched to antiCD20, and (iii) had ≥12 months follow-up after switch. The primary endpoint was occurrence of relapse after switch, secondary endpoints included severe infections (CTCAE grade ≥3).
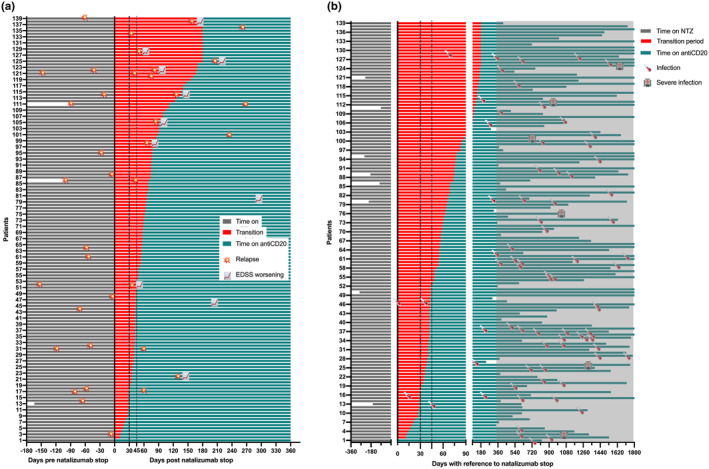
Results: Overall, 139 RMS patients were included (70.5% females, mean age at switch 38.8 years [SD 9.7], mean disease duration at switch 11.3 years [SD 6.2], median duration on NTZ 4.4 years [range: 0.3-16.4], median transition interval 58 days [0-180]). Relapse occurred in 18 patients (12.9%) after NTZ discontinuation. Of those, 11 (61.1%) patients relapsed during the transition interval. No patient with a transition interval below 30 days experienced a relapse, compared to 11.1% and 16.1% with transition intervals of 30-44 days and ≥ 45 days, respectively. In multivariable Cox regression, a transition interval ≥ 45 days predicted a 4.73-fold increased risk of relapse. Over approximately 4 years of follow-up, six severe infections were reported without any noticeable effect of transition interval length. No PML occurred.
Conclusions: Switching from NTZ to antiCD20 is generally both effective and safe. Keeping the transition interval below 30 days provides the optimal balance between preventing recurrent disease activity and ensuring safety.
Keywords: CD20; multiple sclerosis; natalizumab; prediction; risk; switch.
© 2024 The Author(s). European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
Gabriel Bsteh has participated in meetings sponsored by, received speaker honoraria or travel funding from Biogen, BMS/Celgene, Lilly, Merck, Novartis, Roche, Sanofi, and Teva, and received honoraria for consulting Biogen, BMS/Celgene, Novartis, Roche, Sanofi, and Teva. He has received unrestricted research grants from BMS/Celgene and Novartis. Robert Hoepner has received speaker/advisor honorary from Alexion, Almirall, Biogen, BMS/Celgene, Janssen, Merck, Novartis, Roche, Sanofi, and Teva/Mepha. He received research support within the last 5 years from Biogen, BMS/Celgene, Chiesi, Merck, Sanofi, and Roche. He also received research grants from the Swiss MS Society, the SITEM Insel Support Fund and is a member of the Advisory Board of the Swiss and International MS Society. He also serves as deputy editor in chief for Journal of Central Nervous System disease. All conflicts are not related to this work. Jonathan A. Gernert has participated in meetings sponsored by, received travel funding and non‐financial support from Merck. He received a research grant from the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation; SFB/TRR 274, ID 408885537). Klaus Berek has participated in meetings sponsored by and received travel funding or speaker honoraria from Biogen, Merck, Novartis, Roche, Sanofi, and Teva. He is associate editor of Frontiers in Immunology /Neurology, Section Multiple Sclerosis and Neuroimmunology. Christiane Gradl has participated in meetings sponsored by or received honoraria (lectures, consultations) and/or travel funding from Alexion, Almirall, Amgen/Horizon, Biogen, BMS/Celgene, D‐Pharma, Merck, Novartis, Roche, Sanofi, and Teva. Dariia Kliushnikova has participated in meetings sponsored by or received travel funding from Biogen, Merck, Novartis, Roche, Sanofi, and Teva. All conflicts are not related to this work. Anna Damulina has participated in meetings sponsored by, received speaker honoraria or travel funding from Sanofi‐Aventis, Novartis, and Janssen. Gerhard Traxler has participated in meetings sponsored by, received honoraria (lectures, advisory boards, and consultations) or travel funding from Alexion, Amgen/Horizon, Biogen, BMS/Celgene, Janssen, Lilly, Merck, Novartis, Roche, and Sanofi. Fabian Föttinger has nothing to disclose. Sebastian Habernig has nothing to disclose. Nik Krajnc has participated in meetings sponsored by, received speaker honoraria or travel funding from Alexion, BMS/Celgene, Janssen, Merck, Novartis, Roche, and Sanofi. He held a grant for a Multiple Sclerosis Clinical Training Fellowship Programme from the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS). Alejandro Xavier León Betancourt has nothing to disclose. Markus Ponleitner has participated in meetings sponsored by, received speaker or consulting honoraria from Amicus and travel funding from Amicus, Merck, Novartis, and Sanofi. Tobias Zrzavy has participated in meetings sponsored by or received travel funding from Biogen, Merck, Novartis, Roche, and Teva. Florian Deisenhammer has participated in meetings sponsored by or received honoraria for acting as an advisor/speaker for Alexion, Almirall, Biogen, BMS/Celgene, Merck, Novartis, Roche, and Sanofi. His institution received scientific grants from Biogen and Sanofi. Franziska Di Pauli has participated in meetings sponsored by, received honoraria (lectures, advisory boards, and consultations) or travel funding from Bayer, Biogen, BMS/Celgene, Merck, Novartis, Sanofi, Roche, and Teva. Her institution has received research grants from Roche. Joachim Havla has received travel funding, speaker honoraria or nonfinancial support from Alexion, Amgen/Horizon, Bayer, Biogen, BMS/Celgene, Merck, Novartis and Roche, and nonfinancial support of the Sumaira‐Foundation and Guthy‐Jackson Charitable Foundation, all outside the submitted work. He holds research grants from the Friedrich‐Baur‐Stiftung, Amgen/Horizon, Merck and Sanofi. Michael Khalil has received travel funding and speaker honoraria from Bayer, Biogen, Novartis, Merck, Sanofi and Teva, and serves on scientific advisory boards for Biogen, BMS/Celgene, Gilead, Merck, Novartis, and Roche. He received research grants from Biogen, Novartis and Teva. Tania Kümpfel has received speaker honoraria and/or personal fees for advisory boards from Alexion/Astra Zeneca, Amgen/Horizon, Biogen, Chugai, Merck, Novartis, and Roche. The Institution she works for has received compensation for serving as a member of a steering committee from Roche. TK is a site principal investigator in several randomized clinical trials (BMS/Celgene, Novartis, Roche, and Sanofi) and in a randomized clinical trial supported by the BMBf (funding code: 01GM1908E). Her institution has received compensation for clinical trials all outside the present work. Peter Wipfler has participated in meetings sponsored by, received honoraria (lectures, advisory boards, and consultations) or travel funding from Alexion, Amgen/Horizon, Biogen, BMS/Celgene, Janssen, Merck, Novartis, Roche, Sanofi, SQUIBB, and Teva. Andrew Chan has received speakers'/board honoraria from Actelion (Janssen/J&J), Alexion, Almirall, Bayer, Biogen, BMS/Celgene, Merck, Novartis, Roche, Sanofi, and Teva, all for hospital research funds. He received research support from Biogen, CSL Behring, Sanofi, and UCB, the European Union, and the Swiss National Foundation. Thomas Berger has participated in meetings sponsored by and received honoraria (lectures, advisory boards, consultations) from pharmaceutical companies marketing treatments for MS: Allergan, Amgen/Horizon, Bayer, Biogen, Bionorica, BMS, Genesis, GSK, Jazz Pharma, Janssen, MedDay, Merck, Neuraxpharma, Novartis, Octapharma, Roche, Sandoz, Sanofi, Teva and UCB. His institution has received financial support in the past 12 months by unrestricted research grants (Biogen, Bayer, BMS, Merck, Novartis, Roche, Sanofi, Teva) and for participation in clinical trials in multiple sclerosis sponsored by Alexion, Bayer, Biogen, Merck, Novartis, Octapharma, Roche, Sanofi, Teva. Helly Hammer has received speaker/advisor honorary from Biogen, Janssen, Merck, and Teva. She received research support within the last 5 years from Biogen. She received travel grants from Biogen, Janssen, Merck, and Roche. Harald Hegen has participated in meetings sponsored by, received speaker honoraria or travel funding from Amgen/Horizon, Bayer, Biogen, BMS/Celgene, Janssen, Merck, Novartis, Sanofi, Siemens, Teva, and received honoraria for acting as consultant for Biogen, BMS/Celgene, Novartis, Roche, Sanofi, and Teva.
Figures
References
-
- Brown JD, Muston BT, Massey J. Switching from natalizumab to an anti‐CD20 monoclonal antibody in relapsing remitting multiple sclerosis: a systematic review. Mult Scler Relat Disord. 2024;86:105605. - PubMed
-
- Bsteh G, Aicher ML, Walde J, et al. Association of disease‐modifying treatment with outcome in patients with relapsing multiple sclerosis and isolated MRI activity. Neurology. 2024;103:e209752. - PubMed
-
- Thompson AJ, Banwell BL, Barkhof F, et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018;17(2):162‐173. - PubMed
