

Impact of sex differences on patients with neuroendocrine neoplasms during hospital admission
- PMID: 39687054
- PMCID: PMC11648047
- DOI: 10.1177/17588359241292271
Impact of sex differences on patients with neuroendocrine neoplasms during hospital admission
Abstract
Background: Sex disparities are known modifiers of health and disease. In neuroendocrine neoplasms (NENs), sex-based differences have been observed in the epidemiology and treatment-related side effects.
Objectives: To examine sex differences in demographics, diagnoses present during hospital admission, comorbidities, and outcomes of hospital course among hospitalized patients with NENs.
Design: Retrospective analysis.
Methods: A descriptive analysis of sex differences was performed on patients with NENs discharged from U.S. community hospitals in 2019 from the National Inpatient Sample (NIS), Healthcare Cost and Utilization Project, and Agency for Healthcare Research and Quality.
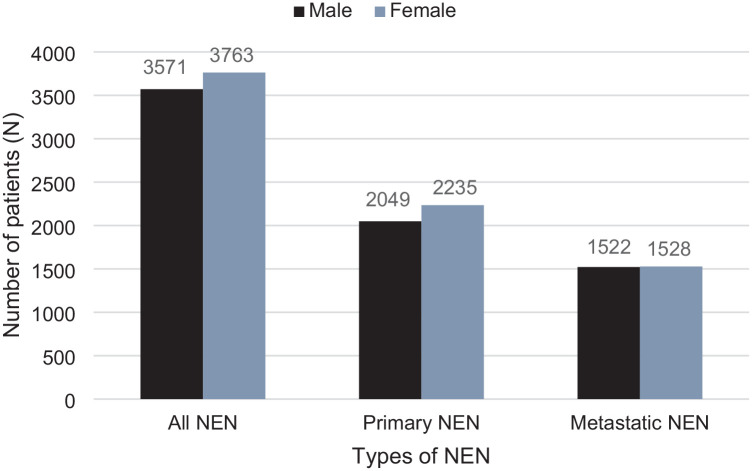
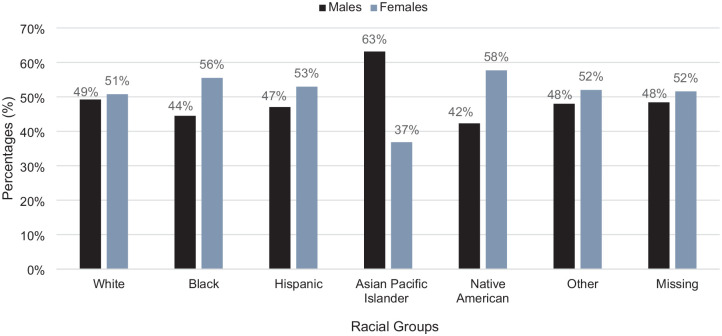
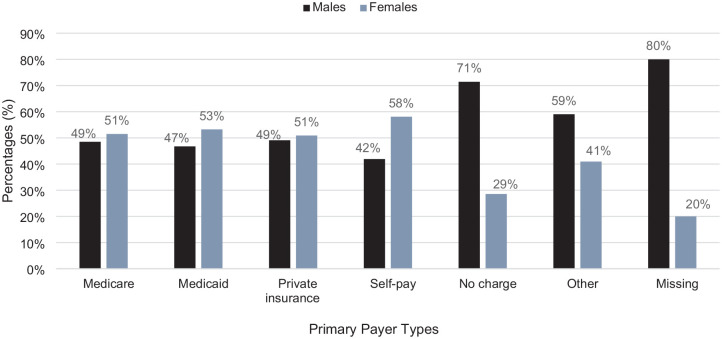
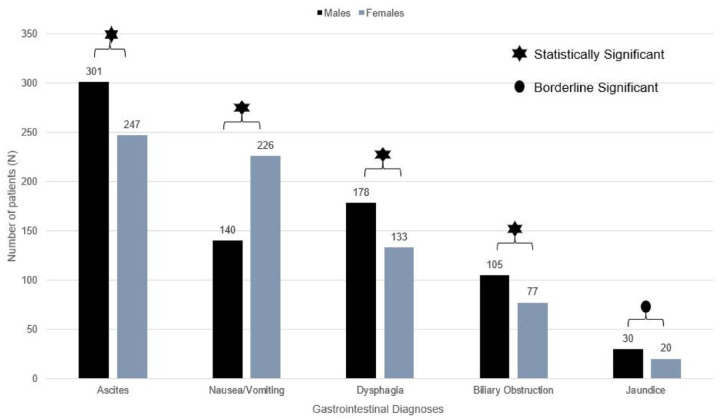
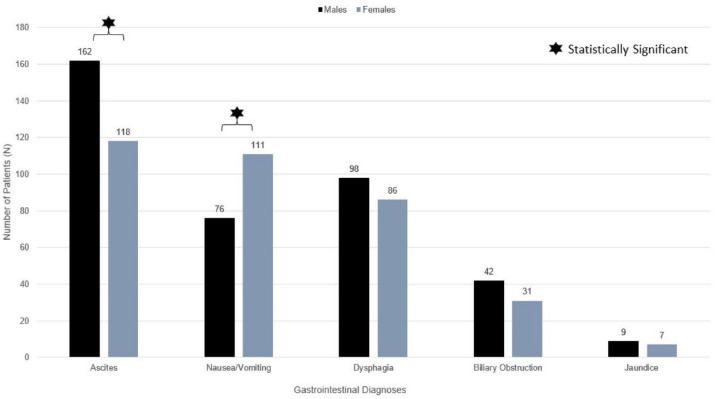
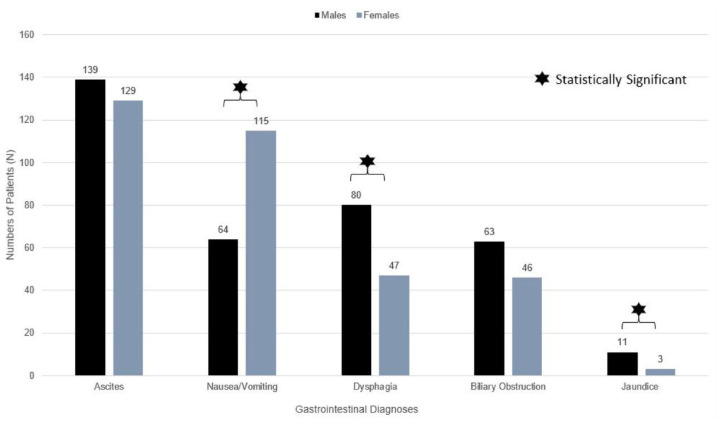
Results: A total of 7334 patients with NENs were identified; 4284 patients had primary NENs, and 3050 patients had metastatic NENs. In total, 48.7% were males and 51.3% were females. Distributions of race and ethnicity, and payer types differed by sex (p < 0.001 and p = 0.027, respectively). For race and ethnicity, there were more females in White, Black, and Native American races, and Hispanic ethnicity. For payer types, female predominance was seen with Medicare, Medicaid, private insurance, and self-pay groups. Sex differences were seen in diagnosis made during hospital stay. In all NENs, oral (p = 0.036) and neurologic (p < 0.001) diagnoses were more common in females; ascites (p = 0.002), dysphagia (p = 0.002), biliary ductal obstruction (p = 0.014), and jaundice (p = 0.048) were more common in males. In primary NENs, ascites (p < 0.001) was male predominant. In metastatic NENs, dysphagia (p = 0.003) and jaundice (p = 0.034) were male predominant, whereas females had more headaches (p < 0.001). Nausea and vomiting were female predominant in all NENs (p < 0.001), primary (p = 0.044), and metastatic (p < 0.001) NENs. For comorbidities, arthropathies (p < 0.001), depression (p < 0.001), hypothyroidism (p < 0.001), other thyroid disorders (p < 0.001), chronic pulmonary disease (p = 0.002), and obesity (p < 0.001) were female predominant.
Conclusion: There were sex differences in the race and ethnicity, payer types, diagnoses present during hospital admission, and comorbidities among the 2019 NIS hospital discharge sample of patients with NENs.
Keywords: adverse effects; comorbidities; diagnoses during hospitalization; healthcare utilization; neuroendocrine neoplasm; neuroendocrine tumors; patient outcomes; sex differences; sex disparities; toxicity; treatment-related side effects.
Plain language summary
Sex differences in patients with neuroendocrine tumors during hospital admission This study explored sex differences in neuroendocrine neoplasms (NENs) using 2019 hospital discharge data. There were variations in demographics, diagnoses, and comorbidities between males and females. Female patients had higher rates of oral and neurologic issues, while males had more ascites, dysphagia, and jaundice. Certain comorbidities like arthritis, depression, hypothyroidism, and obesity were more common in females. Hospital stays and mortality rates did not differ significantly based on sex. In summary, this research highlights distinct sex-related patterns in NENs, shedding light on potential areas for tailored interventions or further investigation.
© The Author(s), 2024.
Conflict of interest statement
Pamela Kunz conflicts for past 12 mo: Research (to institution): Novartis, Rayze Bio Steering Committees (uncompensated): Novartis, Rayze Bio Advisory Boards (uncompensated): Novartis, Exelixis.
Figures
References
-
- Hendifar AE, Marchevsky AM, Tuli R. Neuroendocrine tumors of the lung: current challenges and advances in the diagnosis and management of well-differentiated disease. J Thorac Oncol 2017; 12(3): 425–436. - PubMed
-
- Yao JC, Hassan M, Phan A, et al. One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol 2008; 26(18): 3063–3072. - PubMed
-
- Sorbye H, Strosberg J, Baudin E, et al. Gastroenteropancreatic high-grade neuroendocrine carcinoma. Cancer 2014; 120(18): 2814–2823. - PubMed
LinkOut - more resources
Full Text Sources
