

Blunt trauma-induced complete esophageal avulsion: A case report on surgical intervention and clinical insights
- PMID: 39687515
- PMCID: PMC11648798
- DOI: 10.1016/j.tcr.2024.101117
Blunt trauma-induced complete esophageal avulsion: A case report on surgical intervention and clinical insights
Abstract
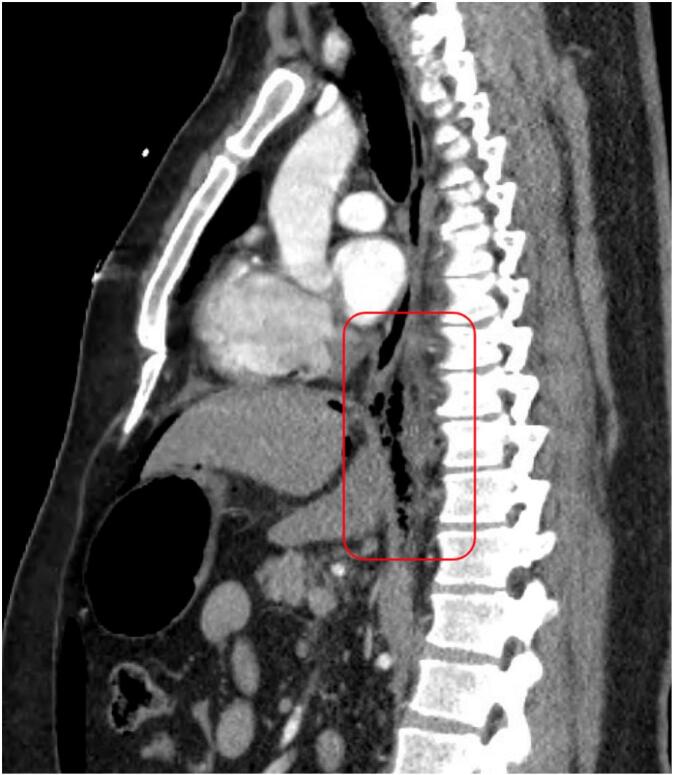
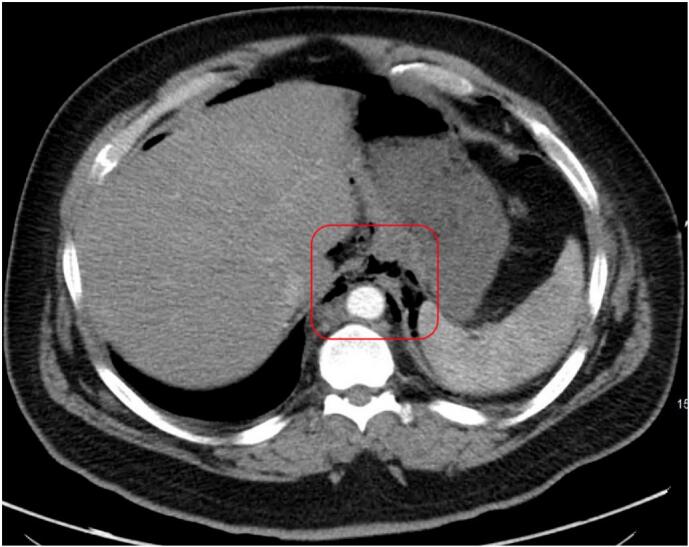
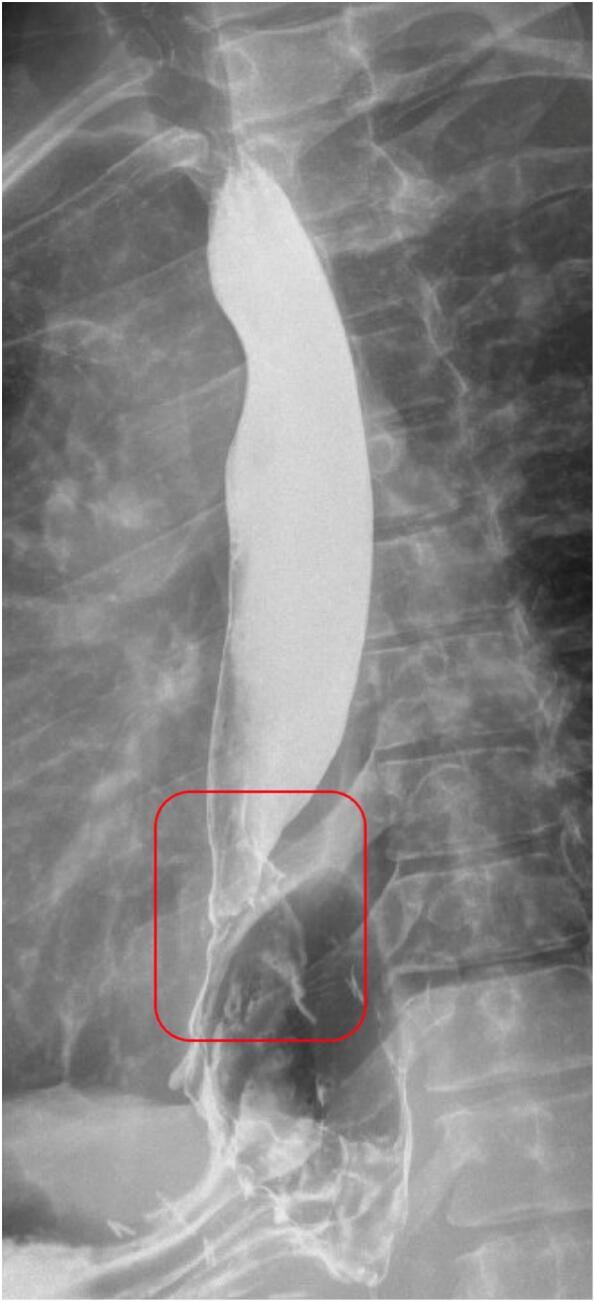
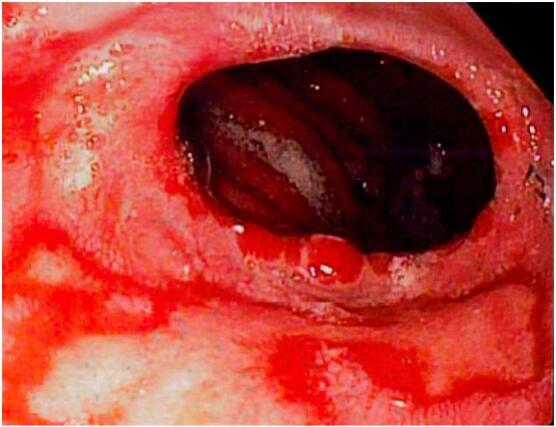
Blunt esophageal injury is an exceptionally rare condition, with complete esophageal avulsion being almost unprecedented in adults. This case study details the clinical presentation, surgical management, and postoperative course of a 50-year-old male who sustained a complete esophageal avulsion following blunt abdominal trauma. The patient presented with increasing abdominal pain two hours after falling while stepping up onto a high truck step, striking his upper abdomen on the step. CT imaging revealed pneumomediastinum and pneumoperitoneum. Emergent exploratory laparotomy and thoracotomy uncovered a complete avulsion of the esophagus from the gastroesophageal junction. The surgical repair involved resection of the damaged esophagus and gastric cardia, an esophagogastric anastomosis using a 25 mm EEA stapler, and the creation of an omental pedicle flap. Postoperative management included antibiotic prophylaxis and intensive care monitoring. Blunt traumatic esophageal injuries, although rare, pose significant diagnostic and therapeutic challenges due to their potential for severe complications such as mediastinitis, sepsis, and multi-organ failure. Prompt recognition of the injury through imaging and clinical assessment is essential for initiating timely surgical intervention. The surgical approach must be meticulously planned to address the complexity of the injury, often requiring a combination of thoracic and abdominal procedures. Additionally, the role of a multidisciplinary team, including surgeons, intensivists, and gastroenterologists, is crucial in managing both the immediate and long-term aspects of patient care. This case emphasizes the necessity for a comprehensive and coordinated treatment strategy to optimize outcomes. It highlights the importance of continued research and education in managing such rare and severe injuries.
Keywords: Blunt trauma; Esophageal avulsion; Esophageal injury; Gastroesophageal junction; Gastroesophageal reflux; Postoperative complications; Surgical repair.
© 2024 The Authors.
Conflict of interest statement
We have nothing to declare.
Figures

Similar articles
-
Isolated gastric perforation following blunt abdominal trauma: A case report.Radiol Case Rep. 2025 Apr 18;20(7):3367-3371. doi: 10.1016/j.radcr.2025.03.044. eCollection 2025 Jul. Radiol Case Rep. 2025. PMID: 40292128 Free PMC article.
-
Could blunt trauma lead to a double lumen esophagus?Int J Surg Case Rep. 2023 Apr;105:108047. doi: 10.1016/j.ijscr.2023.108047. Epub 2023 Mar 24. Int J Surg Case Rep. 2023. PMID: 37003233 Free PMC article.
-
Post-traumatic diaphragmatic rupture with pericardial denudation: A case report.Int J Surg Case Rep. 2021 Jun;83:105970. doi: 10.1016/j.ijscr.2021.105970. Epub 2021 May 15. Int J Surg Case Rep. 2021. PMID: 34029846 Free PMC article.
-
[Esophageal injury following blunt thoracic trauma. A case report and review of the literature].Unfallchirurg. 2012 Dec;115(12):1123-5. doi: 10.1007/s00113-012-2256-2. Unfallchirurg. 2012. PMID: 23052701 Review. German.
-
Combined stomach and duodenal perforating injury following blunt abdominal trauma: a case report and literature review.BMC Surg. 2020 Oct 2;20(1):217. doi: 10.1186/s12893-020-00882-w. BMC Surg. 2020. PMID: 33008373 Free PMC article. Review.
References
-
- Mubang RN, Sigmon DF, Stawicki SP. Esophageal Trauma. StatPearls. StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC.; 2024. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
