

Optimal site of pacemaker lead implantation for persistent atrial standstill guided by electroanatomical mapping following a cox-maze procedure: a case report
- PMID: 39687540
- PMCID: PMC11647587
- DOI: 10.1093/ehjcr/ytae647
Optimal site of pacemaker lead implantation for persistent atrial standstill guided by electroanatomical mapping following a cox-maze procedure: a case report
Abstract
Background: Atrial standstill is characterized by the absence of atrial activity. We report a case of a patient with extensive atrial fibrosis who underwent electrophysiologic study (EPS) and electroanatomical mapping (EAM) to identify surviving atrial sites amenable for pacemaker lead implantation.
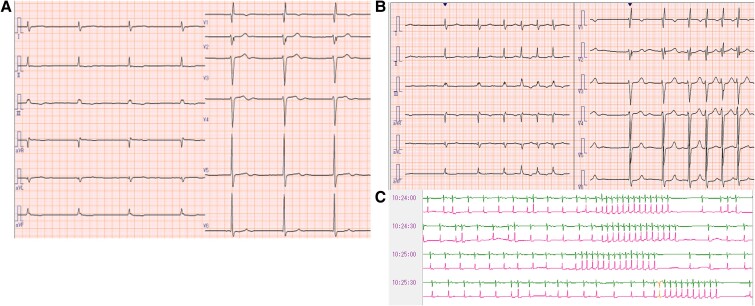
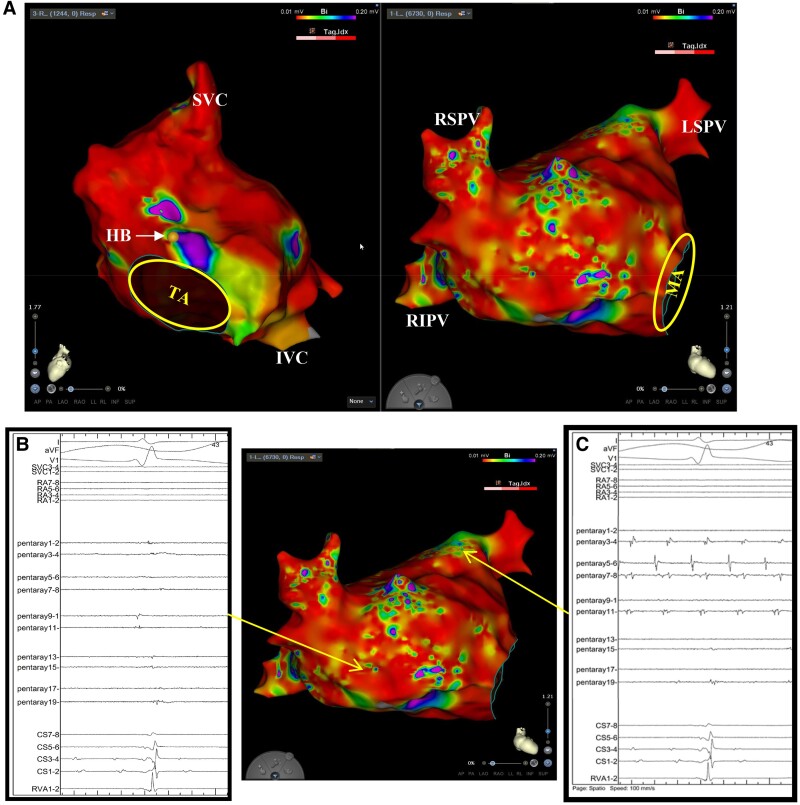
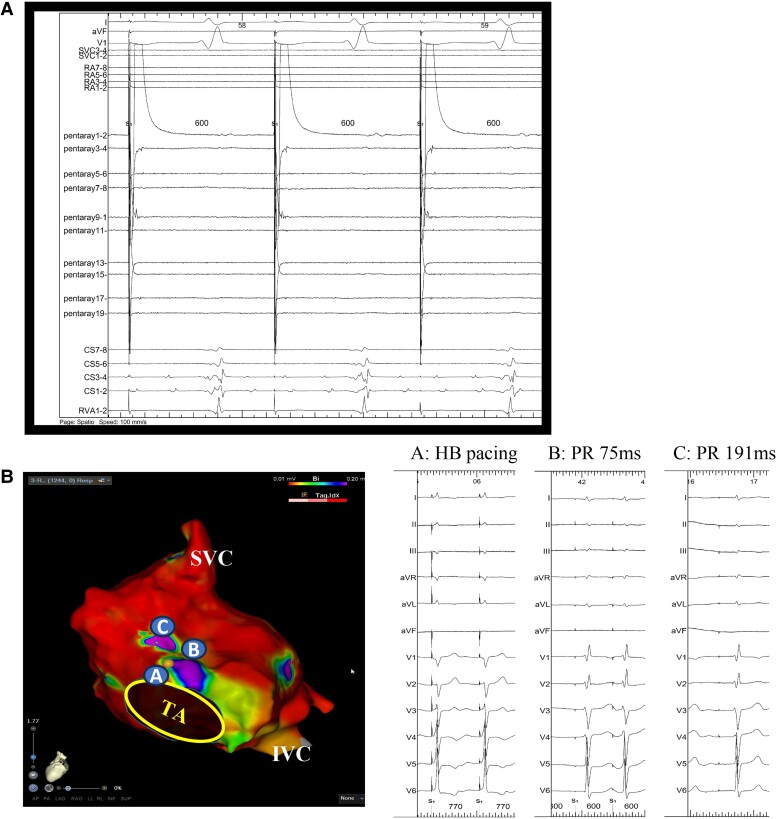
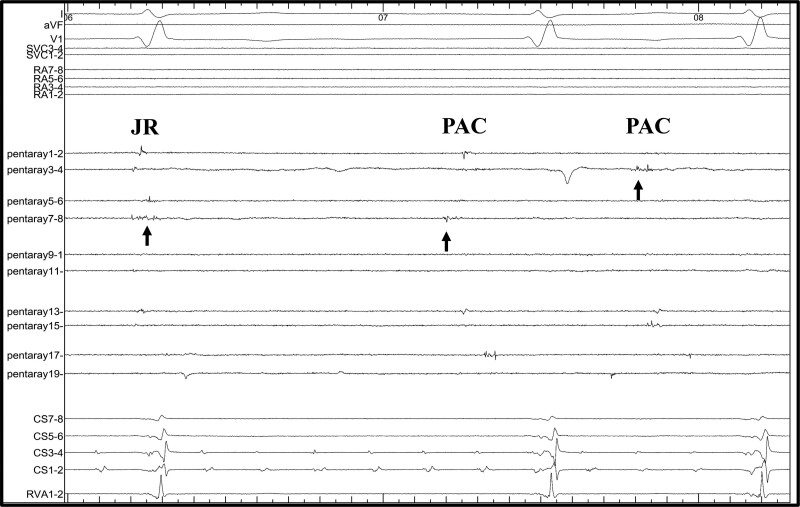
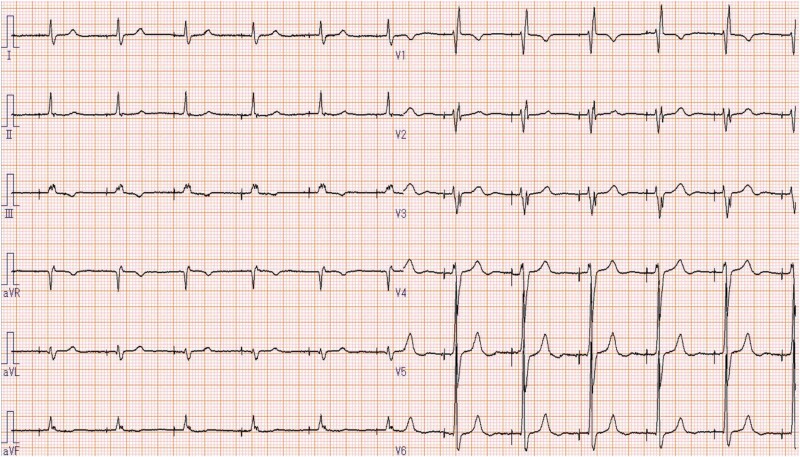
Case summary: A 72-year-old man with persistent atrial fibrillation (AF) and atrial functional mitral regurgitation/tricuspid regurgitation (MR/TR) underwent a Cox-Maze surgery, mitral and tricuspid valve repair, and biatrial plication. He was referred because of post-operative presyncope symptoms. Electrocardiography revealed atrial standstill and junctional rhythm (JR); however, EAM revealed that both atria were almost entirely scarred and isolated fibrillation in left pulmonary veins and coronary sinus. Junctional rhythm retrogradely conducted around an atrioventricular (AV) node and pacing at this area could conduct to the ventricle through the AV node. An atrial pacing lead was implanted at this area, which yielded a QRS wave similar to the own beat. However, the atrial lead voltage was quite low; hence, ventricular pacing lead was implanted to avoid a future occurrence of pacing failure.
Discussion: This report demonstrates the benefits of EPS and EAM in informing optimal pacemaker implantation for patients with extensive scar in atrium.
Keywords: Atrial fibrillation; Case report; Electroanatomical mapping; Electrophysiologic study; Pacemaker lead implantation.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Society of Cardiology.
Conflict of interest statement
Conflict of interest: None declared.
Figures

References
-
- Kakuta T, Fukushima S, Minami K, Kawanoto N, Tadokoro N, Saiki Y, et al. Incidence of and risk factors for pacemaker implantation after the modified Cryo-Maze procedure for atrial fibrillation. J Thorac Cardiovasc Surg 2023;166:755–766.e1. - PubMed
-
- Soni LK, Cedola SR, Cogan J, Jiang J, Yang J, Takayama H, et al. Right atrial lesions do not improve the efficacy of a complete left atrial lesion set in the surgical treatment of atrial fibrillation, but they do increase procedural morbidity. J Thorac Cardiovasc Surg 2013;145:356–361. - PMC - PubMed
-
- Alfieri O, De Bonis M, Lapenna E, Agricola E, Quarti A, Maisano F. “The “clover technique” as a novel approach for correction of post-traumatic tricuspid regurgitation.” J Thorac Cardiovasc Surg 2003;126:75–79. - PubMed
Publication types
LinkOut - more resources
Full Text Sources