

Using trauma video review to search for the Goldilocks pre-activation time
- PMID: 39687555
- PMCID: PMC11647353
- DOI: 10.1136/tsaco-2024-001588
Using trauma video review to search for the Goldilocks pre-activation time
Abstract
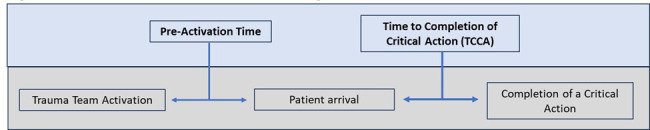
Objectives: We sought to determine the optimal time to pre-activation for trauma team activation that resulted in maximum team efficiency, measured by the time to complete critical actions (TCCAs) during resuscitation. We hypothesized that there exists a time window for trauma team pre-activation that minimizes TCCA.
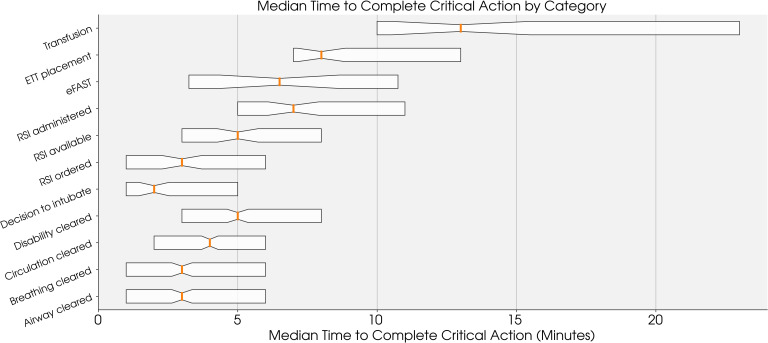
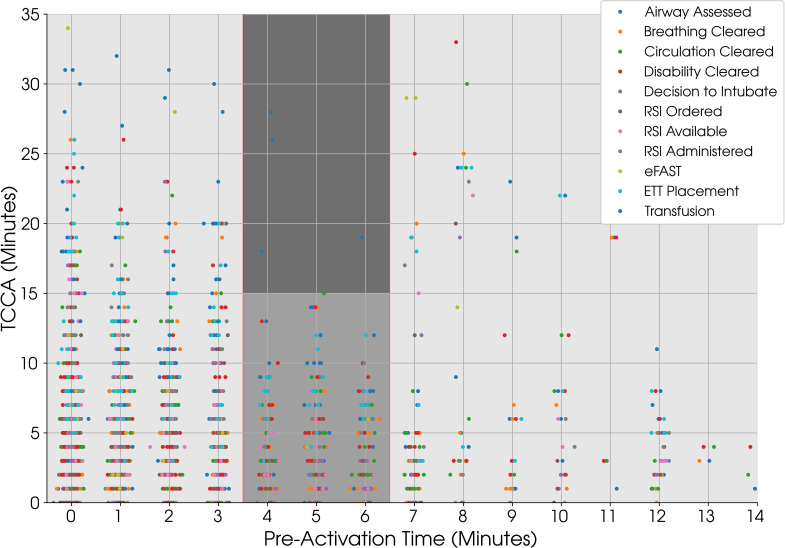
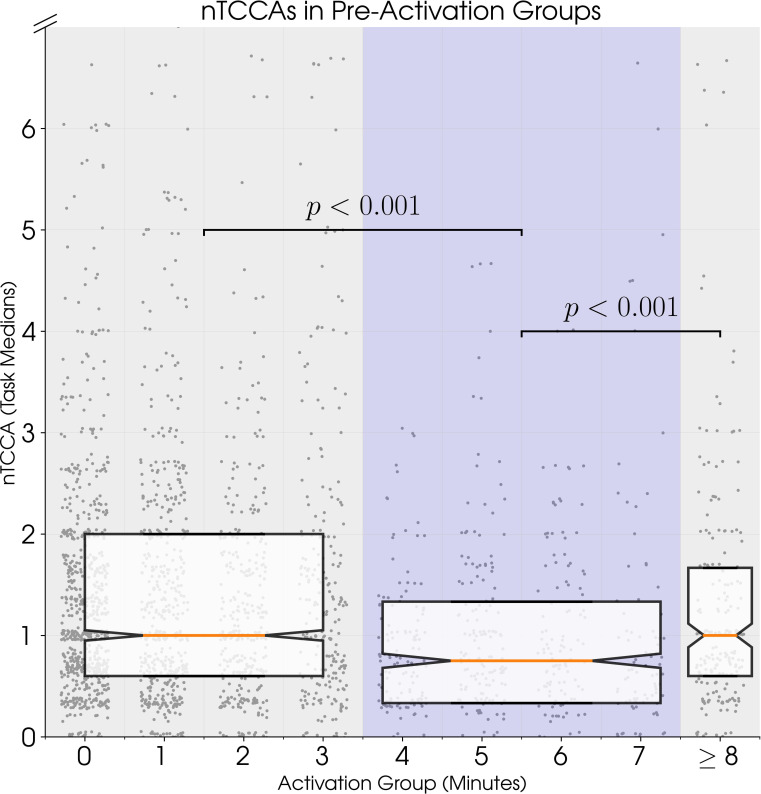
Methods: This is an exploratory retrospective analysis of video-reviewed traumas at a level 1 trauma center from January 1, 2018 to 28 February, 2022 that received the highest trauma team activation and had a pre-arrival notification. A total of 11 TCCA categories were calculated using video timestamps. To compare TCCAs from different categories, normalized TCCAs (nTCCAs) were calculated by dividing each TCCA by the median time of its category. Pre-activation times were categorized into three groups: long pre-activation (≥8 min), mid pre-activation (≥4 and ≤7 min), and short pre-activation (≥0 and ≤4).
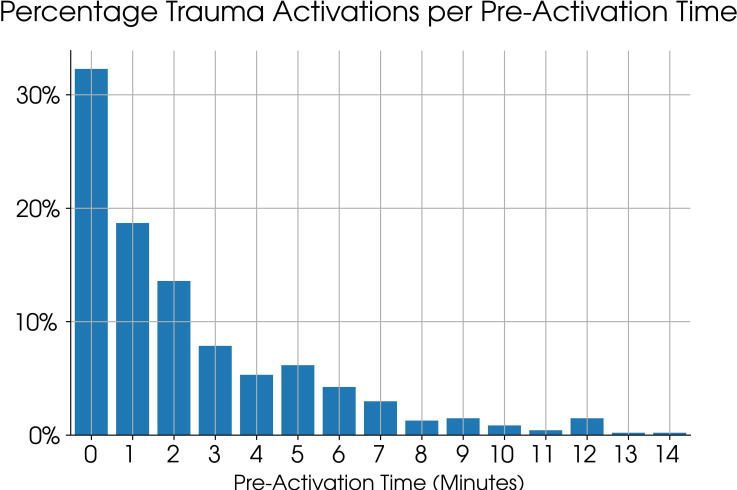
Results: There were 466 video-recorded level 1 trauma activations, which resulted in 2334 TCCAs. Of the 466 activations, 152 occured on the patient's arrival (0 min pre-activation). The majority (425) of patients had a pre-activation time of <7 min. Pre-activation of 4-6 min resulted in all but blood transfusion TCCAs being <15 min. Furthermore, mid pre-activation category corresponded to the most efficient trauma teams, with nTCCAs significantly shorter (median=0.75 (IQR 0.3-1.3)) than long (median=1 (IQR 0.6-2)) or short activation groups (median=1 (IQR 0.6-1.6)). A greater proportion of nTCCAs were shorter than their category median in the mid pre-activation category compared with long and short categories (59.1% vs 48.3% and 40%, respectively; p<0.01).
Conclusions: In this exploratory study, a pre-activation time of 4-7 min is associated with the best team efficiency as measured by TCCAs during trauma team activations. This timeframe may be an optimal window for trauma team activations but needs prospective and external validation.
Level of evidence: Level 4 retrospective exploratory study.
Keywords: emergency medical services; emergency treatment; video.
Copyright © Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
None declared.
Figures
References
-
- Elm E von, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ . 2007;335:806–8. doi: 10.1136/bmj.39335.541782.AD. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials