

Smartwatch ECG and artificial intelligence in detecting acute coronary syndrome compared to traditional 12-lead ECG
- PMID: 39687687
- PMCID: PMC11648863
- DOI: 10.1016/j.ijcha.2024.101573
Smartwatch ECG and artificial intelligence in detecting acute coronary syndrome compared to traditional 12-lead ECG
Abstract
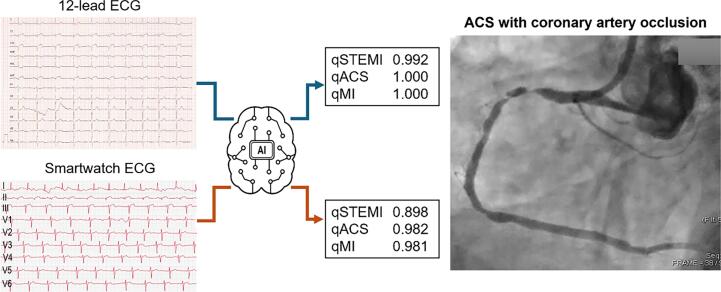
Background: Acute coronary syndromes (ACS) require prompt diagnosis through initial electrocardiograms (ECG), but ECG machines are not always accessible. Meanwhile, smartwatches offering ECG functionality have become widespread. This study evaluates the feasibility of an image-based ECG analysis artificial intelligence (AI) system with smartwatch-based multichannel, asynchronous ECG for diagnosing ACS.
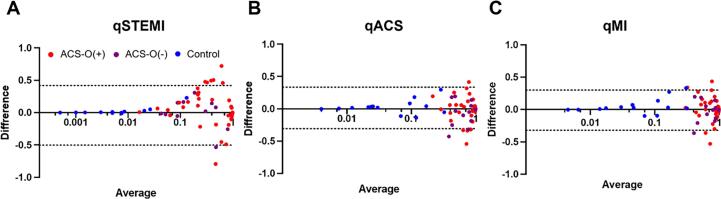
Methods: Fifty-six patients with ACS and 15 healthy participants were included, and their standard 12-lead and smartwatch-based 9-lead ECGs were analyzed. The ACS group was categorized into ACS with acute total occlusion (ACS-O(+), culprit stenosis ≥ 99 %, n = 44) and ACS without occlusion (ACS-O(-), culprit stenosis 70 % to < 99 %, n = 12) based on coronary angiography. A deep learning-based AI-ECG tool interpreting 2-dimensional ECG images generated probability scores for ST-elevation myocardial infarction (qSTEMI), ACS (qACS), and myocardial injury (qMI: troponin I > 0.1 ng/mL).
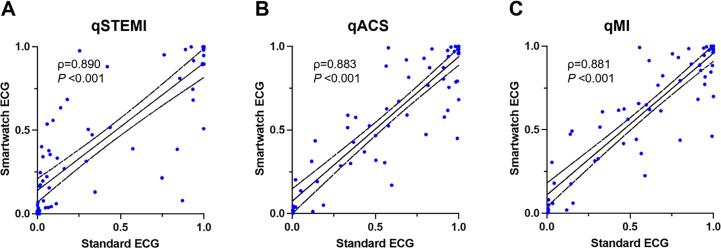
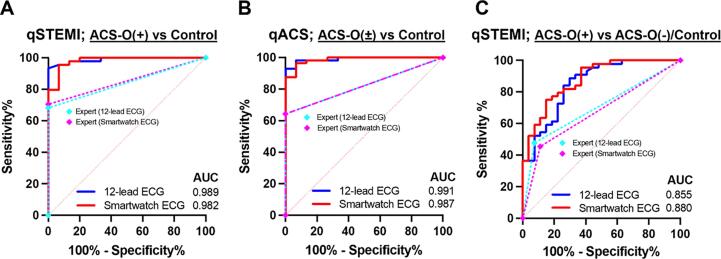
Results: The AI-driven qSTEMI, qACS, and qMI demonstrated correlation coefficients of 0.882, 0.874, and 0.872 between standard and smartwatch ECGs (all P < 0.001). The qACS score effectively distinguished ACS-O(±) from control, with AUROC for both ECGs (0.991 for standard and 0.987 for smartwatch, P = 0.745). The AUROC of qSTEMI in identifying ACS-O(+) from control was 0.989 and 0.982 with 12-lead and smartwatch (P = 0.617). Discriminating ACS-O(+) from ACS-O(-) or control presented a slight challenge, with an AUROC for qSTEMI of 0.855 for 12-lead and 0.880 for smartwatch ECGs (P = 0.352).
Conclusion: AI-ECG scores from standard and smartwatch-based ECGs showed high concordance with comparable diagnostic performance in differentiating ACS-O(+) and ACS-O(-). With increasing accessibility smartwatch accessibility, they may hold promise for aiding ACS diagnosis, regardless of location.
Keywords: Acute Coronary Syndrome; Artificial Intelligence; Diagnostic Performance; Smartwatch ECG.
© 2024 The Author(s).
Conflict of interest statement
The authors declare the following financial interests/personal relationships which may be considered as potential competing interests: [Youngjin Cho reports financial support was provided by Korea Health Industry Development Institute. Joonghee Kim reports a relationship with ARPI Inc. that includes: employment. Youngjin Cho reports a relationship with ARPI Inc. that includes: employment. If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper].
Figures
References
-
- Ibanez B., James S., Agewall S., Antunes M.J., Bucciarelli-Ducci C., Bueno H., et al. 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC) Eur Heart J. 2018;39:119–177. - PubMed
-
- O'Gara P.T., Kushner F.G., Ascheim D.D., Casey D.E., Jr., Chung M.K., de Lemos J.A., et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the american college of cardiology foundation/american heart association task force on practice guidelines. J Am Coll Cardiol. 2013;61:e78–e140. - PubMed
-
- Writing Committee M., Lawton J.S., Tamis-Holland J.E., Bangalore S., Bates E.R., Beckie T.M., et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the american college of cardiology/american heart association joint committee on clinical practice guidelines. J Am Coll Cardiol. 2022;79:e21–e129. - PubMed
-
- Ranasinghe I., Rong Y., Du X., Wang Y., Gao R., Patel A., et al. System barriers to the evidence-based care of acute coronary syndrome patients in China: qualitative analysis. Circ Cardiovasc Qual Outcomes. 2014;7:209–216. - PubMed
LinkOut - more resources
Full Text Sources
