

Efficacy, safety, and quality of life 4 years after valoctocogene roxaparvovec gene transfer for severe hemophilia A in the phase 3 GENEr8-1 trial
- PMID: 39687929
- PMCID: PMC11647608
- DOI: 10.1016/j.rpth.2024.102615
Efficacy, safety, and quality of life 4 years after valoctocogene roxaparvovec gene transfer for severe hemophilia A in the phase 3 GENEr8-1 trial
Abstract
Background: Valoctocogene roxaparvovec, an adeno-associated virus-mediated gene therapy for severe hemophilia A, enables endogenous factor (F)VIII expression and provides bleed protection.
Objectives: Determine valoctocogene roxaparvovec durability, efficacy, and safety 4 years after treatment.
Methods: In the phase 3 GENEr8-1 trial, 134 adult male persons with severe hemophilia A without inhibitors and previously using FVIII prophylaxis received a 6 × 1013 vg/kg infusion of valoctocogene roxaparvovec. Efficacy endpoints included annualized bleed rate, annualized FVIII infusion rate, FVIII activity, and the Haemophilia-Specific Quality of Life Questionnaire for Adults. Adverse events and immunosuppressant use were assessed. Change from baseline was assessed after participants discontinued prophylaxis (scheduled for week 4).
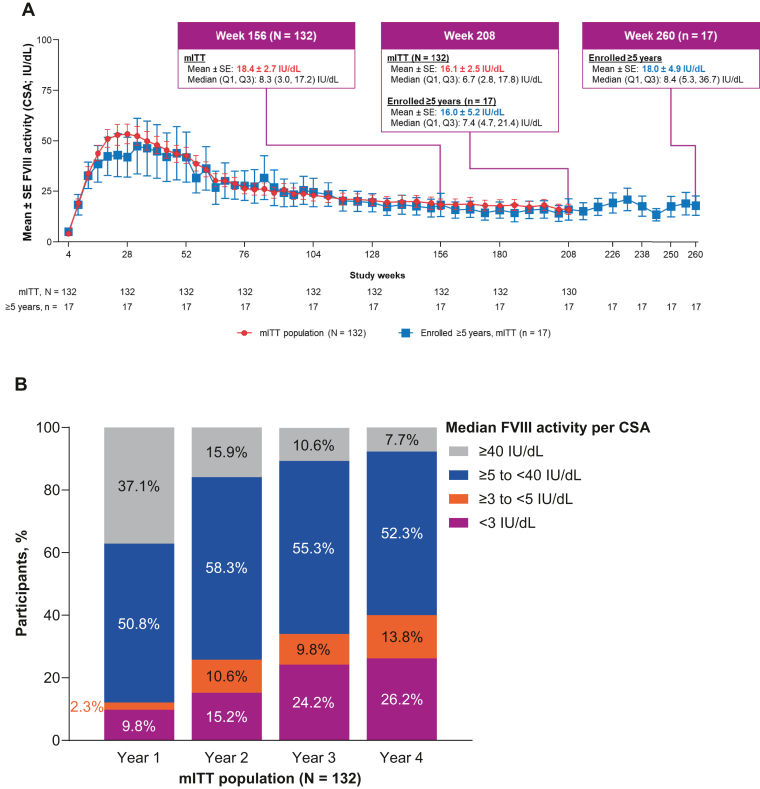
Results: Median follow-up was 214.3 weeks; 2 participants discontinued since the previous data cutoff. Declines from baseline in mean treated annualized bleed rate (-82.6%; P < .0001) and annualized FVIII infusion rate (-95.5%; P < .0001) were maintained from previous years in the primary analysis population of 112 participants who enrolled from a noninterventional study. During year 4, 81 of 110 rollover participants experienced 0 treated bleeds. Week 208 mean and median chromogenic FVIII activity were 16.1 IU/dL and 6.7 IU/dL, respectively, in 130 modified intention-to-treat participants. Seven participants resumed prophylaxis since the previous data cutoff. Mean change from baseline to week 208 in Haemophilia-Specific Quality of Life Questionnaire for Adults Total Score (P < .0001) remained clinically meaningful for modified intention-to-treat participants. Alanine aminotransferase elevation was the most common adverse event during year 4 (56/131 participants); none required immunosuppressants.
Conclusion: Valoctocogene roxaparvovec provides persistent FVIII expression, hemostatic control, and health-related quality of life improvements with no new safety signals.
Keywords: adeno-associated virus; clinical trial; gene therapy; hemophilia A; quality of life.
© 2024 The Authors.
Figures



References
-
- Srivastava A., Santagostino E., Dougall A., Kitchen S., Sutherland M., Pipe S.W., et al. WFH guidelines for the management of hemophilia, 3rd edition. Haemophilia. 2020;26(Suppl 6):1–158. - PubMed
-
- Mahlangu J., Oldenburg J., Paz-Priel I., Negrier C., Niggli M., Mancuso M.E., et al. Emicizumab prophylaxis in patients who have hemophilia A without inhibitors. N Engl J Med. 2018;379:811–822. - PubMed
