

A novel computational model ITHCS for enhanced prognostic risk stratification in ESCC by correcting for intratumor heterogeneity
- PMID: 39690882
- PMCID: PMC11652613
- DOI: 10.1093/bib/bbae631
A novel computational model ITHCS for enhanced prognostic risk stratification in ESCC by correcting for intratumor heterogeneity
Abstract
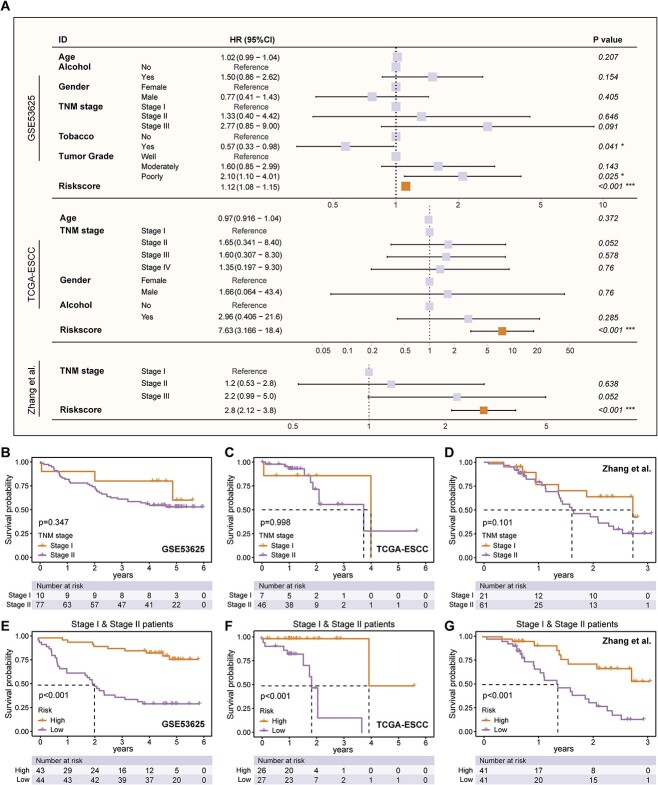
Intratumor heterogeneity significantly challenges the accuracy of existing prognostic models for esophageal squamous cell carcinoma (ESCC) by introducing biases related to the varied genetic and molecular landscapes within tumors. Traditional models, relying on single-sample, single-region bulk RNA sequencing, fall short of capturing the complexity of intratumor heterogeneity. To fill this gap, we developed a computational model for intratumor heterogeneity corrected signature (ITHCS) by employing both multiregion bulk and single-cell RNA sequencing to pinpoint genes that exhibit consistent expression patterns across different tumor regions but vary significantly among patients. Utilizing these genes, we applied multiple machine-learning algorithms for sophisticated feature selection and model construction. The ITHCS model significantly outperforms existing prognostic indicators in accuracy and generalizability, markedly reducing sampling biases caused by intratumor heterogeneity. This improvement is especially notable in the prognostic assessment of early-stage ESCC patients, where the model exhibits exceptional predictive power. Additionally, we found that the risk score based on ITHCS may be associated with epithelial-mesenchymal transition characteristics, indicating that high-risk patients may exhibit a diminished efficacy to immunotherapy.
Keywords: esophageal squamous cell carcinoma; intra-tumor heterogeneity; machine learning; prognostic prediction; sampling bias.
© The Author(s) 2024. Published by Oxford University Press.
Figures






References
MeSH terms
Substances
Grants and funding
- 82072557/National Natural Science Foundation of China
- 2021YFC2500900/National Key Research and Development Program of China
- 20XD1402300/Program of Shanghai Academic Research Leader from Science and Technology Commission of Shanghai Municipality
- 2022JC023/Novel Interdisciplinary Research Project from Shanghai Municipal Health Commission
- YG2023ZD04/Interdisciplinary Program of Shanghai Jiao Tong University
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
