

Reconstruction of a body wall defect using diaphragm lateralisation and advancement, latissimus dorsi, and internal and external abdominal oblique muscle flaps in a cat
- PMID: 39691671
- PMCID: PMC11650495
- DOI: 10.1177/20551169241285257
Reconstruction of a body wall defect using diaphragm lateralisation and advancement, latissimus dorsi, and internal and external abdominal oblique muscle flaps in a cat
Abstract
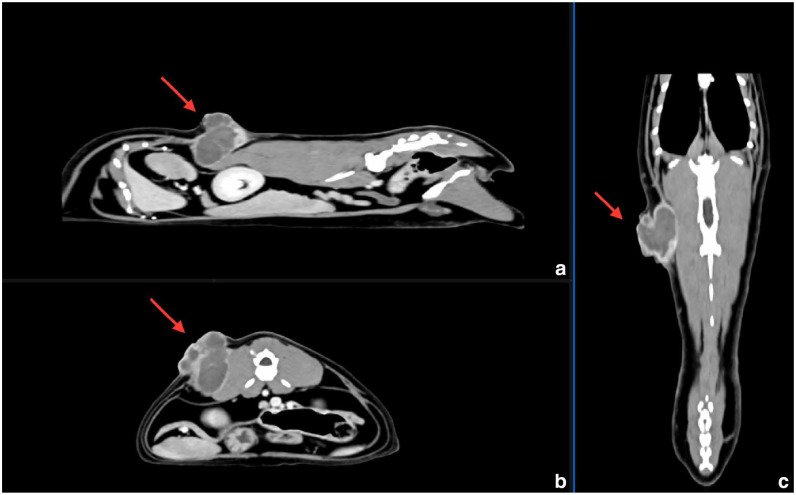
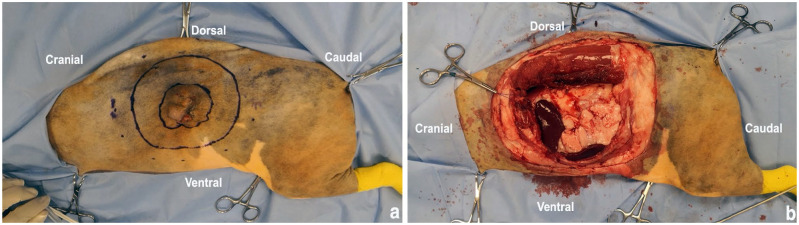
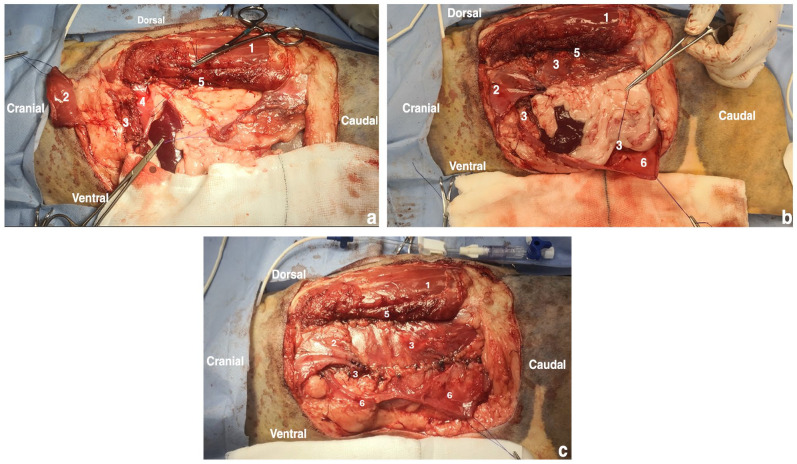
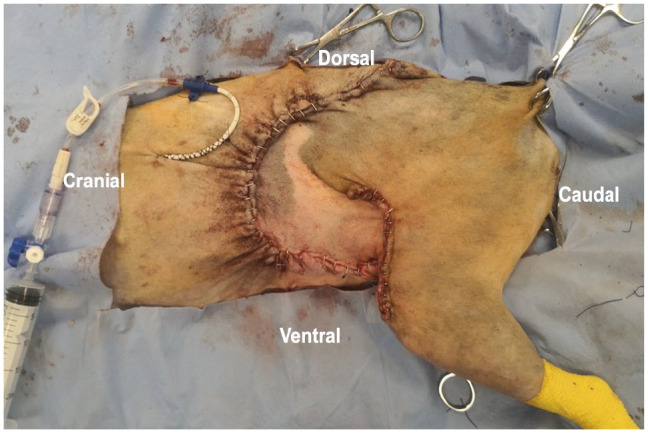
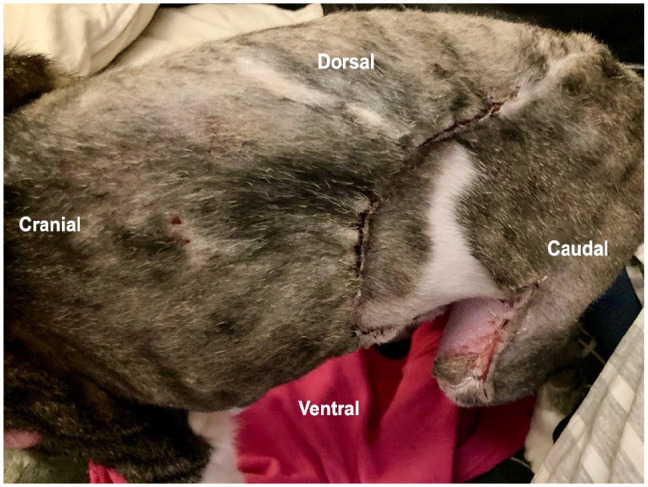
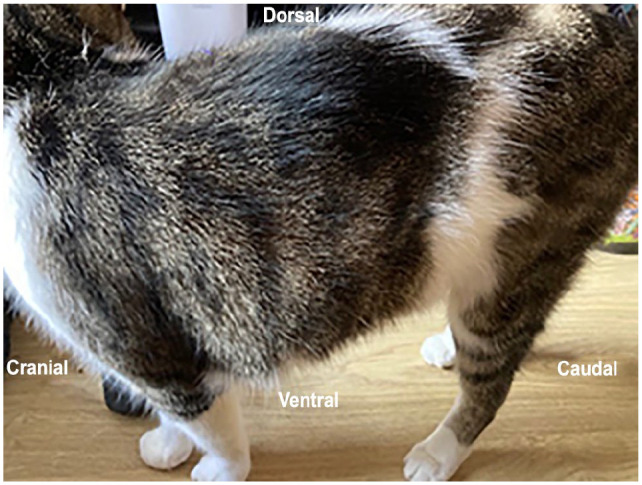
Case summary: A cat aged 12 years and 7 months was referred to a multidisciplinary hospital for investigation of feline injection site sarcoma (FISS) on the left thoracolumbar region. A CT examination of the mass revealed a multi-lobulated mass affecting the body wall, extending from the level of lumbar vertebrae L2 to L4. The mass was excised with 5 cm lateral margins, including resection of the 13th left rib, the caudal edge of the latissimus dorsi (LD) muscle, full-thickness abdominal wall and sections of the lumbar epaxial muscles. To reconstruct the defect, a combination of muscle flaps was used. This included diaphragmatic advancement and lateralisation, rotation of the LD, and creation of transposition flaps from the internal abdominal oblique and external abdominal oblique muscles, ensuring closure without tension. Skin closure required mobilising an inguinal flank fold flap. The cat was discharged from hospital 3 days postoperatively. Histopathology confirmed a diagnosis of FISS with clean wide margins. A gradual return to normal activity and complete healing of the surgical site was reported on follow-up, with one minor complication related to the skin flap (bruising at the base of the inguinal flank fold flap).
Relevance and novel information: This report describes the use of the aforementioned combination of muscle flaps to close a major abdominal wall defect in a cat with an excellent outcome. Practitioners can consider this technique when planning tissue reconstruction after FISS resection.
Keywords: FISS; Injection site sarcoma; body wall defect; muscle flap; reconstruction.
© The Author(s) 2024.
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Martano M, Morello E, Buracco P. Feline injection-site sarcoma: past, present and future perspectives. Vet J 2011; 188: 136–141. - PubMed
-
- Srivastav A, Kass PH, McGill LD, et al. Comparative vaccine-specific and other injectable-specific risks of injection-site sarcomas in cats. J Am Vet Med Assoc 2012; 241: 595–602. - PubMed
-
- Couto SS, Griffey SM, Duarte PC, et al. Feline vaccine-associated fibrosarcoma: morphologic distinctions. Vet Pathol 2002; 39: 33–41. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous