

Integrating omics data and machine learning techniques for precision detection of oral squamous cell carcinoma: evaluating single biomarkers
- PMID: 39691710
- PMCID: PMC11649677
- DOI: 10.3389/fimmu.2024.1493377
Integrating omics data and machine learning techniques for precision detection of oral squamous cell carcinoma: evaluating single biomarkers
Abstract
Introduction: Early detection of oral squamous cell carcinoma (OSCC) is critical for improving clinical outcomes. Precision diagnostics integrating metabolomics and machine learning offer promising non-invasive solutions for identifying tumor-derived biomarkers.
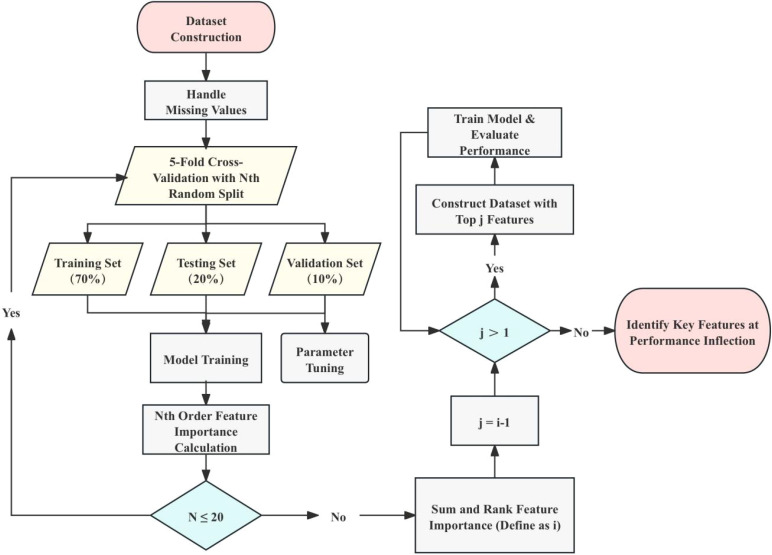
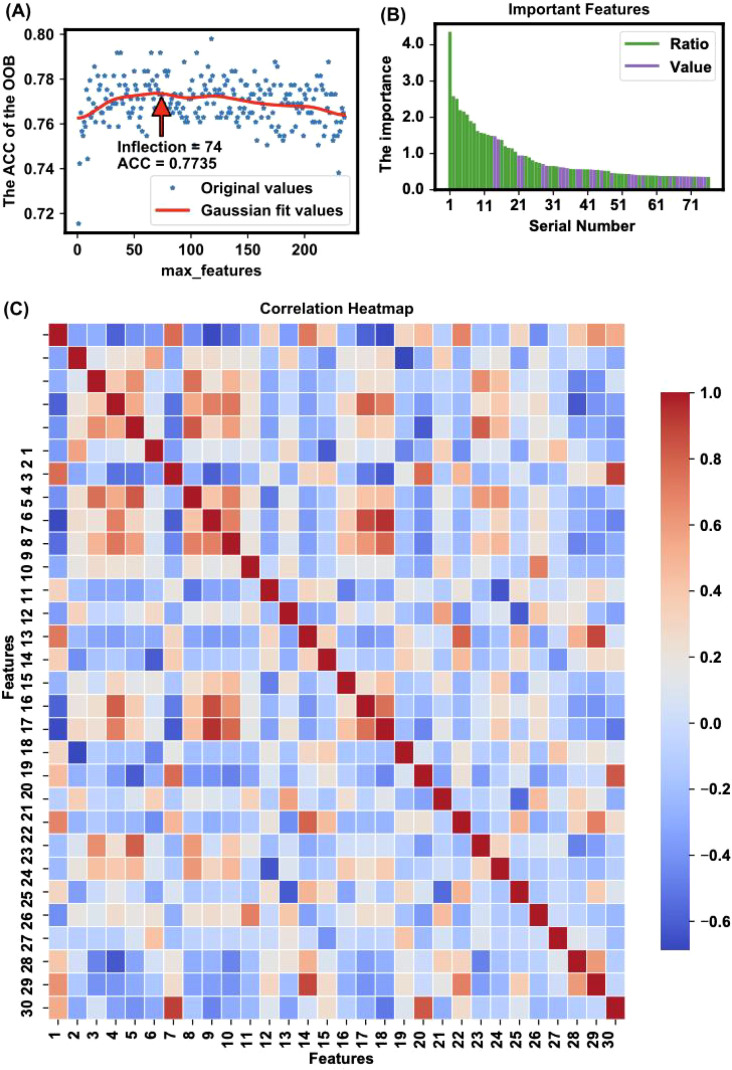
Methods: We analyzed a multicenter public dataset comprising 61 OSCC patients and 61 healthy controls. Plasma metabolomics data were processed to extract 29 numerical and 47 ratio features. The Extra Trees (ET) algorithm was applied for feature selection, and the TabPFN model was used for classification and prediction.
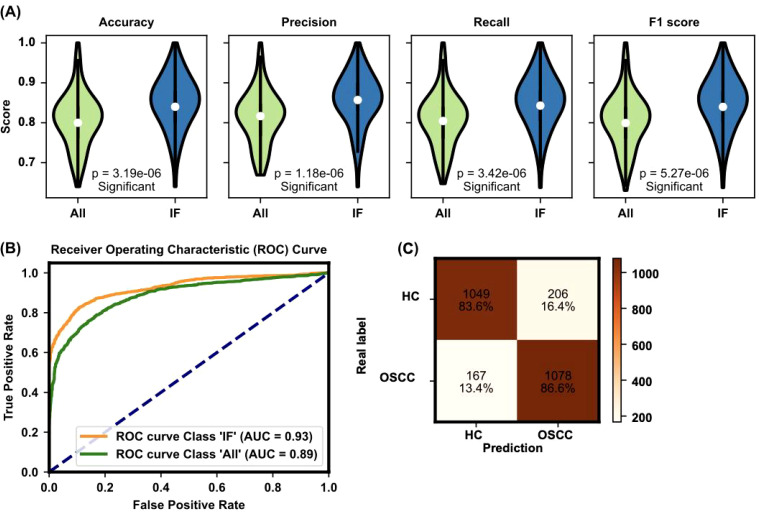
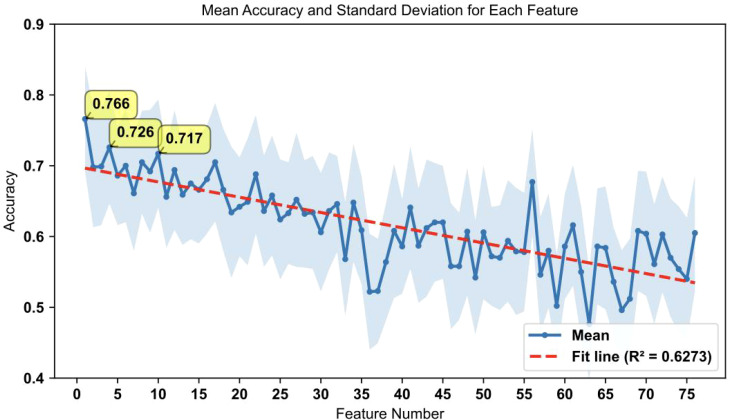
Results: The model achieved an area under the curve (AUC) of 93% and an overall accuracy of 76.6% when using top-ranked individual biomarkers. Key metabolic features significantly differentiated OSCC patients from healthy controls, providing a detailed metabolic fingerprint of the disease.
Discussion: Our findings demonstrate the utility of integrating omics data with advanced machine learning techniques to develop accurate, non-invasive diagnostic tools for OSCC. The study highlights actionable metabolic signatures that have potential applications in personalized therapeutics and early intervention strategies.
Keywords: feature selection; machine learning; oral squamous cell carcinoma; personalized therapy; precision metabolomics.
Copyright © 2024 Sun, Cheng, Wei, Luo and Liu.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures

Similar articles
-
Exploring a Novel Screening Method for Patients with Oral Squamous Cell Carcinoma: A plasma Metabolomics Analysis.Kobe J Med Sci. 2018 Sep 11;64(1):E26-E35. Kobe J Med Sci. 2018. PMID: 30282895 Free PMC article.
-
Applying Machine Learning for Enhanced MicroRNA Analysis: A Companion Risk Tool for Oral Squamous Cell Carcinoma in Standard Care Incisional Biopsy.Biomolecules. 2024 Apr 9;14(4):458. doi: 10.3390/biom14040458. Biomolecules. 2024. PMID: 38672474 Free PMC article.
-
Pairwise analysis of gene expression for oral squamous cell carcinoma via a large-scale transcriptome integration.J Cell Mol Med. 2024 Oct;28(20):e70153. doi: 10.1111/jcmm.70153. J Cell Mol Med. 2024. PMID: 39470584 Free PMC article.
-
Emerging histological and serological biomarkers in oral squamous cell carcinoma: Applications in diagnosis, prognosis evaluation and personalized therapeutics (Review).Oncol Rep. 2023 Dec;50(6):213. doi: 10.3892/or.2023.8650. Epub 2023 Oct 20. Oncol Rep. 2023. PMID: 37859591 Free PMC article. Review.
-
Application of metabolomics in oral squamous cell carcinoma.Oral Dis. 2024 Sep;30(6):3719-3731. doi: 10.1111/odi.14895. Epub 2024 Feb 20. Oral Dis. 2024. PMID: 38376209 Review.
References
-
- Polachini GM, de Castro TB, Smarra L, Henrique T, de Paula C, Severino P, et al. . Plasma metabolomics of oral squamous cell carcinomas based on NMR and MS approaches provides biomarker identification and survival prediction. Sci Rep. (2023) 13:8588. doi: 10.1038/s41598-023-34808-2 - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical