

Trends for Admission, Mortality and Emergency Surgery in Upper Gastrointestinal Bleeding: A Study of Eight Years of Admissions in a Tertiary Care Hospital
- PMID: 39691837
- PMCID: PMC11651075
- DOI: 10.2147/IJGM.S496966
Trends for Admission, Mortality and Emergency Surgery in Upper Gastrointestinal Bleeding: A Study of Eight Years of Admissions in a Tertiary Care Hospital
Abstract
Introduction: Most studies have shown a declining incidence of upper gastrointestinal bleeding (UGIB) in recent years. Data regarding mortality were controversial; in non-variceal bleeding, the increasing age of the population, increased use of anti-thrombotic and anticoagulant therapy in patients with cardiovascular diseases, and the use of non-steroidal anti-inflammatory drugs are counterbalanced by the progress in endoscopic therapy with stable mortality.
Material and method: We performed a retrospective, cross-sectional study that included patients admitted with UGIB in Clinical Emergency Hospital Craiova during 2013-2020.
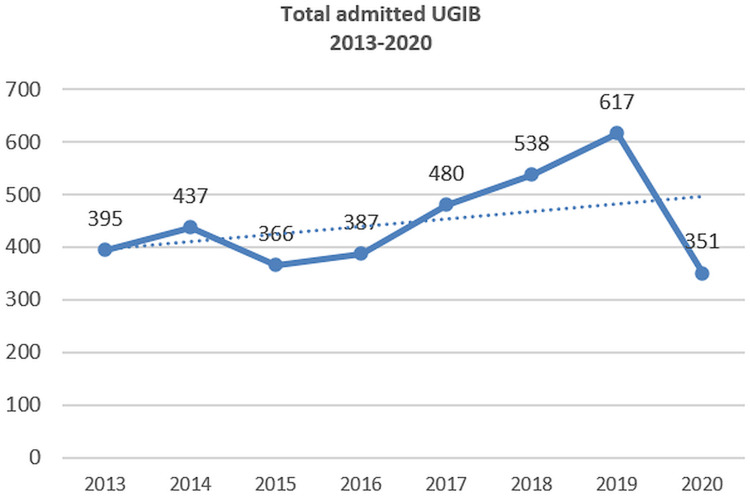
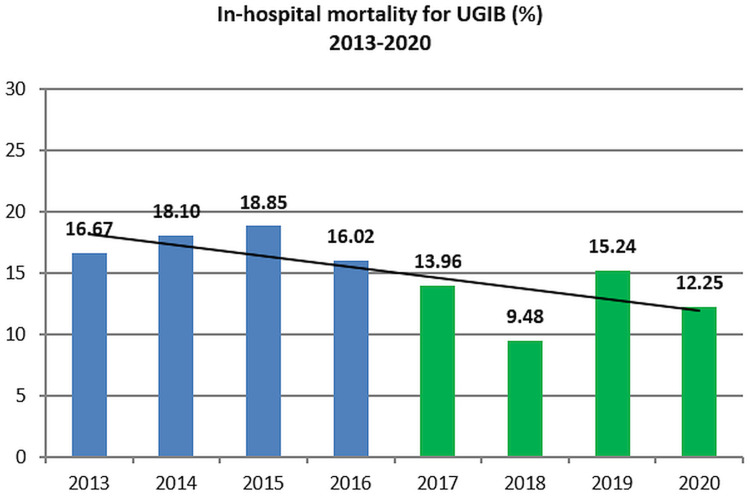
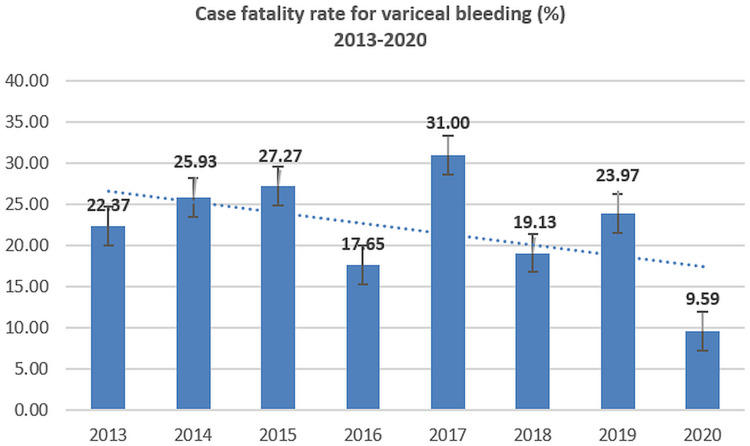
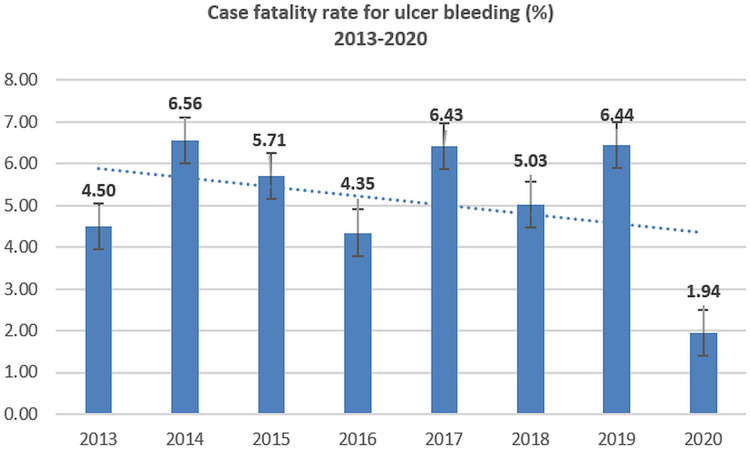
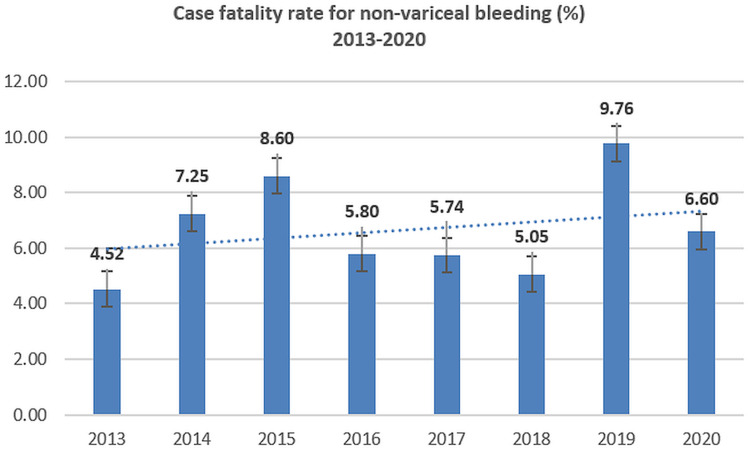
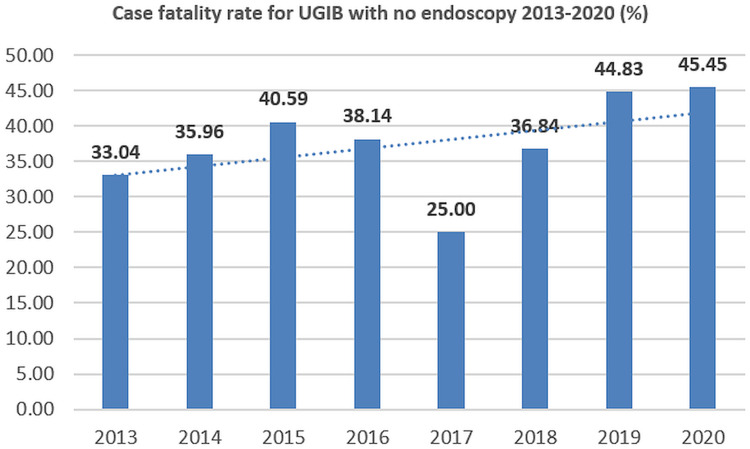
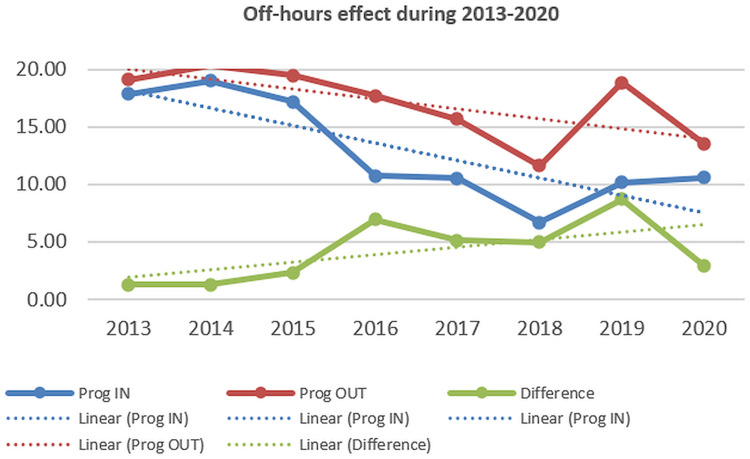
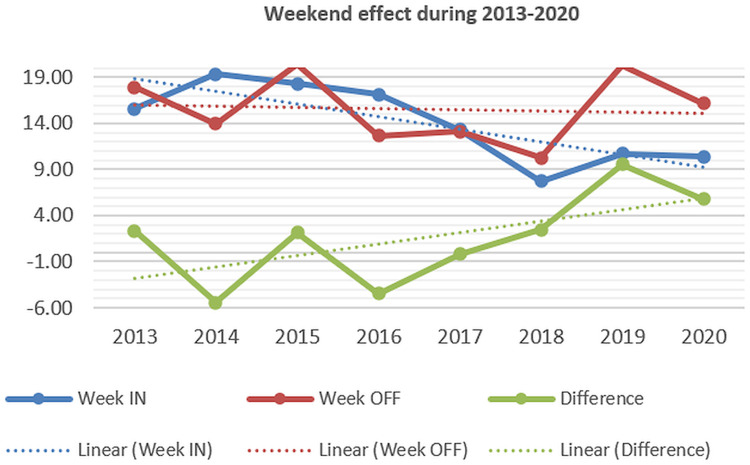
Results: 3571 patients with UGIB were selected; a trend toward increased admission for UGIB from 2013 to 2019 was noted, with a significant decrease in 2020. Non-variceal bleeding remains the most frequent form, with a slight increase in variceal bleeding, of Mallory-Weiss syndrome and angiodysplasia, and a 3-fold decrease for unknown etiology bleeding (with no endoscopy performed) during the 2017-2020 period as compared to 2013-2016. There was a trend toward decreased mortality, with lower mortality in 2017-2020 (12.83%) compared to 2013-2016 (17.41%). The mortality for variceal bleeding and peptic ulcer bleeding has declined, but mortality for non-variceal bleeding has slightly increased during 2013-2020. Mortality has decreased in admissions during regular hours/after hours and weekdays/weekends, but the difference (off-hours and weekend effects) had increased. The percentage of endoscopies performed in the first 24 hours after admission and the rate of therapeutic endoscopy increased during 2017-2020; the median time between admission and endoscopy was 17.0 hours during 2017-2020 and 59.1 hours during 2013-2016. The proportion of patients who needed emergency surgery for uncontrolled bleeding has significantly declined since 2013-2015, with an average value of 1% in the last 5 years of the study.
Conclusion: Increased admissions for UGIB, with lower mortality, especially for peptic ulcer bleeding and variceal bleeding were noted; higher percentages of therapeutic endoscopies and endoscopies performed during the first 24 hours after admission were also recorded.
Keywords: emergency surgery; endoscopy; peptic ulcer bleeding; upper gastrointestinal bleeding.
© 2024 Cazacu et al.
Conflict of interest statement
The author(s) declare(s) that there is no conflict of interest regarding the publication of this paper.
Figures
Similar articles
-
The Reduction of After-Hours and Weekend Effects in Upper Gastro-intestinal Bleeding Mortality During the COVID-19 Pandemic Compared to the Pre-Pandemic Period.J Multidiscip Healthc. 2023 Oct 26;16:3151-3165. doi: 10.2147/JMDH.S427449. eCollection 2023. J Multidiscip Healthc. 2023. PMID: 37908341 Free PMC article.
-
[Clinical epidemiological characteristics and change trend of upper gastrointestinal bleeding over the past 15 years].Zhonghua Wei Chang Wai Ke Za Zhi. 2017 Apr 25;20(4):425-431. Zhonghua Wei Chang Wai Ke Za Zhi. 2017. PMID: 28440524 Chinese.
-
Urgent endoscopy in elderly patients with non-variceal upper gastrointestinal bleeding.Wideochir Inne Tech Maloinwazyjne. 2012 Dec;7(4):246-50. doi: 10.5114/wiitm.2011.28907. Epub 2012 May 31. Wideochir Inne Tech Maloinwazyjne. 2012. PMID: 23362423 Free PMC article.
-
Acute upper gastrointestinal bleeding (UGIB) - initial evaluation and management.Best Pract Res Clin Gastroenterol. 2013 Oct;27(5):633-8. doi: 10.1016/j.bpg.2013.09.002. Epub 2013 Sep 25. Best Pract Res Clin Gastroenterol. 2013. PMID: 24160923 Review.
-
Diagnosis and therapy of non-variceal upper gastrointestinal bleeding.World J Gastrointest Pharmacol Ther. 2015 Nov 6;6(4):172-82. doi: 10.4292/wjgpt.v6.i4.172. World J Gastrointest Pharmacol Ther. 2015. PMID: 26558151 Free PMC article. Review.
References
-
- Zhao Y, Encinosa W.Hospitalizations for gastrointestinal bleeding in 1998 and 2006: statistical brief #65.In:Healthcare Cost and Utilization Project (HCUP) Statistical Briefs [Internet].Rockville (MD):Agency for Healthcare Research and Quality (US);2008.Dec.Available from.http://www.ncbi.nlm.nih.gov/books/NBK54562/. - PubMed
-
- Estevinho MM, Pinho R, Fernandes C, et al. Diagnostic and therapeutic yields of early capsule endoscopy and device-assisted enteroscopy in the setting of overt GI bleeding: a systematic review with meta-analysis. Gastrointest Endosc. 2022;95(4):610–625.e9. doi:10.1016/j.gie.2021.12.009 Epub 2021 Dec 21. PMID: 34952093. - DOI - PubMed
LinkOut - more resources
Full Text Sources
