

Diagnostic Accuracy of Chest X-ray Computer-Aided Detection Software for Detection of Prevalent and Incident Tuberculosis in Household Contacts
- PMID: 39692469
- PMCID: PMC11912973
- DOI: 10.1093/cid/ciae528
Diagnostic Accuracy of Chest X-ray Computer-Aided Detection Software for Detection of Prevalent and Incident Tuberculosis in Household Contacts
Abstract
Background: World Health Organization (WHO) tuberculosis (TB) screening guidelines recommend computer-aided detection (CAD) software for chest radiograph (CXR) interpretation. However, studies evaluating their diagnostic and prognostic accuracy are limited.
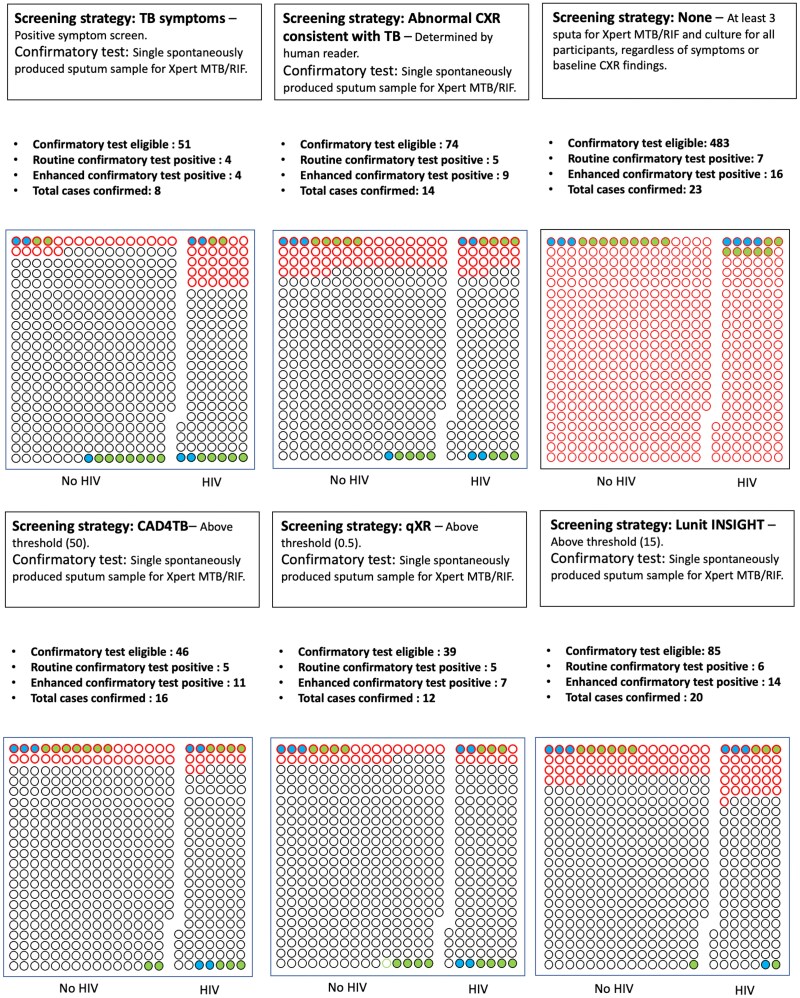
Methods: We conducted a prospective cohort study of household contacts of rifampicin-resistant TB in South Africa. Participants underwent baseline CXR and sputum investigation (routine [single spontaneous] and enhanced [additionally 2-3 induced]) for prevalent TB and follow-up for incident TB. Three CXR-CAD software products (CAD4TBv7.0, qXRv3.0.0, and Lunit INSIGHT v3.1.4.111) were compared. We evaluated their performance to detect routine and enhanced prevalent and incident TB, comparing performance with blood tests (Xpert MTB host-response, erythrocyte sedimentation rate, C-reactive protein, QuantiFERON) in a subgroup.
Results: 483 participants were followed up for 4.6 years (median). There were 23 prevalent (7 routinely diagnosed) and 38 incident TB cases. The AUC ROCs (95% CIs) to identify prevalent TB for CAD4TBv7.0, qXRv3.0.0, and Lunit INSIGHT v3.1.4.111 were .87 (.77-.96), .88 (.79-.97), and .91 (.83-.99), respectively. More than 30% with scores above recommended CAD thresholds who were bacteriologically negative on routine baseline sputum were subsequently diagnosed by enhanced sputum investigation or during follow-up. The AUC performance of baseline CAD to identify incident cases ranged between .60 and .65. Diagnostic performance of CAD for prevalent TB was superior to blood testing.
Conclusions: Our findings suggest that the potential of CAD-CXR screening for TB is not maximized as a high proportion of those above current thresholds, but with a negative routine confirmatory sputum, have true TB disease that may benefit intervention.
Keywords: active case finding; asymptomatic; chest X-ray; computer-aided detection; tuberculosis.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. S. V. K. and M. R. report Free installation and use of CAD software licenses to FIND as an institution as part of research and evaluation studies. S. V. K. reports receiving consulting fees from FIND and the International Organization of Migration. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures




References
-
- World Health Organization . Global tuberculosis report 2024. Geneva, Switzerland: World Health Organization, 2024.
-
- Nguyen TBP, Nguyen TA, Luu BK, et al. . A comparison of digital chest radiography and Xpert® MTB/RIF in active case finding for tuberculosis. Int J Tuberc Lung Dis 2020; 24:934–40. - PubMed
-
- Madhani F, Maniar RA, Burfat A, et al. . Automated chest radiography and mass systematic screening for tuberculosis. Int J Tuberc Lung Dis 2020; 24:665–73. - PubMed
-
- Onozaki I, Law I, Sismanidis C, Zignol M, Glaziou P, Floyd K. National tuberculosis prevalence surveys in Asia, 1990–2012: an overview of results and lessons learned. Trop Med Int Health 2015; 20:1128–45. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
