

Pulmonary involvement in newly diagnosed and untreated rheumatoid arthritis and psoriatic arthritis: a prospective longitudinal study
- PMID: 39692860
- PMCID: PMC11655587
- DOI: 10.1007/s00296-024-05751-w
Pulmonary involvement in newly diagnosed and untreated rheumatoid arthritis and psoriatic arthritis: a prospective longitudinal study
Abstract
Objectives: To longitudinally assesses pulmonary involvement in newly diagnosed rheumatoid arthritis (RA) and psoriatic arthritis (PsA) patients over a 12-months follow-up. To identify biomarkers and establish a diagnostic algorithm for monitoring pulmonary changes.
Methods: Newly diagnosed RA and PsA patients were examined with clinical and laboratory assessments, pulmonary function tests (PFT), and chest radiography (CXR) at three-months intervals for one year.
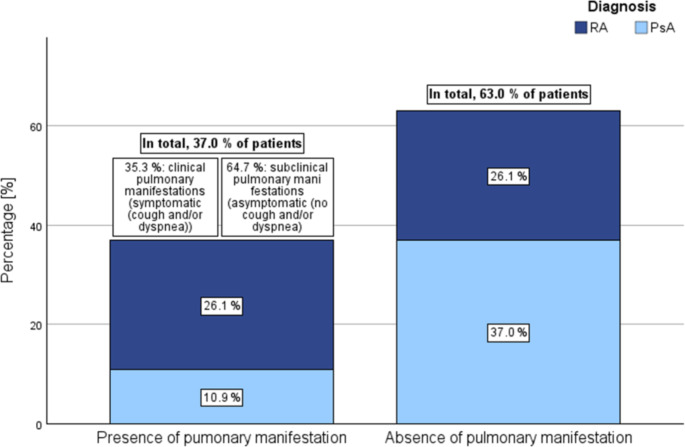
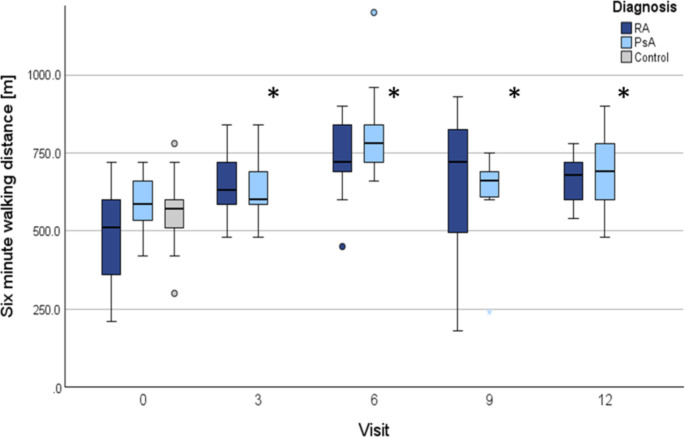
Results: The study enrolled 50 patients (26 RA, 24 PsA) and 26 controls. At baseline, 37.0% of arthritis patients (50.0% RA, 22.7% PsA) exhibited radiographic pulmonary involvement, with 64.7% being asymptomatic. No association was observed between CXR and PFTs. Reduced pathological breathing width was noted in 64.0% of patients (RA 69.2%, PsA 58.3%) and 23.1% of controls (p < .001). Thoracic excursion and lung auscultation showed no differences. During follow-up, PFT and physical examination findings remained stable. Mean CRP levels significantly decreased in RA patients from 23.5 mg/l (± 33.6; 95% CI: 9.9-37.1) to 2.7 mg/L (± 3.4; 95% CI: 1.0-4.3), and in PsA patients from 13.3 mg/L (± 18.0; 95% CI: 5.7-20.9) to 8.1 mg/L (± 16.2; 95% CI: 0.1-16.2) (p < .001). Additionally, significant reductions in disease activity scores and improvements in six-minute walking distance were observed (p < .001). No associations were identified between PFT outcomes, disease activity, or rheumatological medications throughout the disease course.
Conclusion: Our study underscores the prevalence of significant, predominantly asymptomatic pulmonary involvement in newly diagnosed RA and PsA patients. The lack of correlation between pulmonary function, disease activity, and medication during disease progression suggests that reducing arthritic disease activity does not necessarily mitigate the risk or severity of pulmonary involvement. Finally, our finding underscore the need for more sensitive biomarkers and optimized monitoring strategies.
Keywords: Autoimmune Diseases; Follow-up Studies; Lung Diseases; Psoriatic Arthritis; Rheumatoid Arthritis; Thoracic Radiography.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: The study was conducted in accordance with the Declaration of Helsinki and has been reviewed and approved by the ethics committee of the University Hospital Bonn, Germany (reference number: 209/18). Written informed consent was obtained from every patient prior to inclusion in the study. Competing interests: The authors have no competing interests to declare that are relevant to the content of this article. Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research. Consent to participate: Informed consent was obtained from all subjects before enrollment. Patient consent for publication: Not applicable. Note on related congress abstracts and publication: This manuscript is an original work and has not been published or submitted elsewhere, in part or in whole. A related publication addressed the baseline findings of this cohort: Schäfer VS, Winter L, Skowasch D, et al. Exploring pulmonary involvement in newly diagnosed rheumatoid arthritis and psoriatic arthritis: A single-center study. Rheumatol Int. 2024 Oct;44(10):1975–1986. doi: https://doi.org/10.1007/s00296-024-05685-3 . Epub 2024 Aug 21. PMID: 39167172; PMCID: PMC11392970. While the prior study focused on baseline examination results, the current manuscript presents a longitudinal analysis of follow-up data from the same cohort, specifically examining the progression of pulmonary involvement in patients with rheumatoid arthritis and psoriatic arthritis. A summary of baseline findings is included for contextual clarity, resulting in minor overlap with the previous publication. In cases of overlap, the prior study is appropriately cited to acknowledge its contribution.
Figures

References
-
- Turesson C, O’Fallon WM, Crowson CS et al (2002) Occurrence of extraarticular disease manifestations is associated with excess mortality in a community based cohort of patients with rheumatoid arthritis. J Rhuematol 29:62–67 - PubMed
-
- Figus FA, Piga M, Azzolin I et al (2021) Rheumatoid arthritis: Extra-articular manifestations and comorbidities. Autoimmun rev 20:102776. 10.1016/j.autrev.2021.102776 - PubMed
-
- Kelly C, Iqbal K, Iman-Gutierrez L et al (2016) Lung involvement in inflammatory rheumatic diseases. Best Pract Res Clin Rheumatol 30:870–888. 10.1016/j.berh.2016.10.004 - PubMed
-
- West S (2018) Clinical Overview of Rheumatoid Arthritis. Lung Disease in Rheumatoid Arthritis. Humana, Cham, pp 1–18
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
