

Endoscopic-assisted versus open fronto-orbital distraction for unicoronal craniosynostosis: morphometric and technique considerations
- PMID: 39692920
- PMCID: PMC11655604
- DOI: 10.1007/s00381-024-06662-8
Endoscopic-assisted versus open fronto-orbital distraction for unicoronal craniosynostosis: morphometric and technique considerations
Abstract
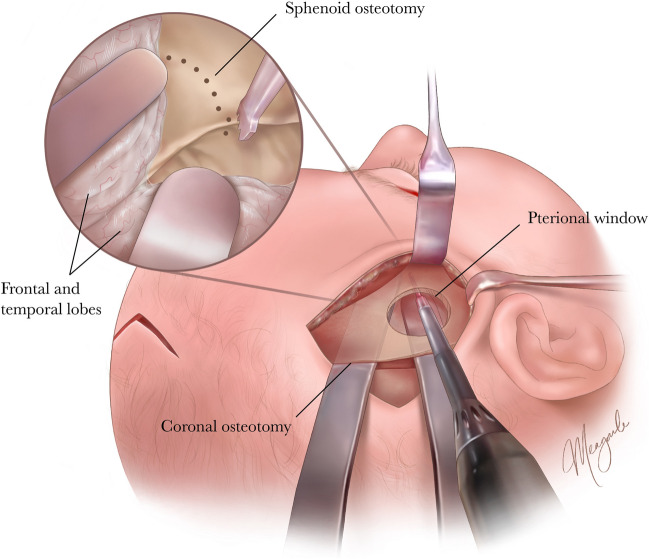
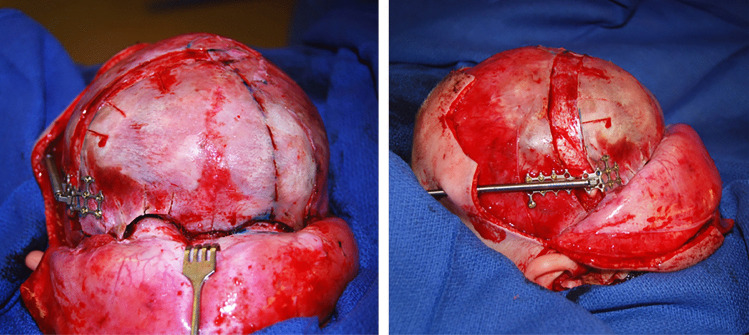
Introduction: In an effort to maximize benefit and minimize morbidity when performing fronto-orbital distraction osteogenesis (FODO) for unilateral coronal synostosis (UCS), we have transitioned to an endoscopic-assisted approach ("endo-FODO"). This study compares photogrammetric outcomes of patients who underwent FODO via an endoscopic-assisted versus open approach.
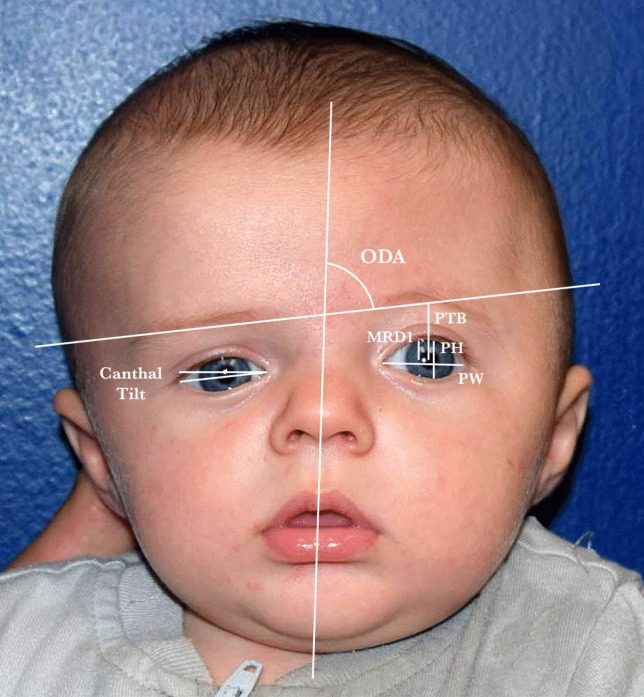
Methods: We retrospectively reviewed patients treated for UCS from 2013 to 2023. Photogrammetric outcomes at one to three years postoperatively were compared between patients who underwent endo-FODO and age- and sex-matched controls who underwent open FODO. Differences between pre- and postoperative periorbital symmetry ratios, canthal tilt symmetry, and orbital dystopia angle (ODA) were calculated.
Results: Twenty patients (ten per group) underwent surgery at a mean age of 6.1 ± 1.8 and 5.4 ± 1.1 months (p = 0.426) and were photographed at 1.6 ± 0.9 and 1.8 ± 0.9 years (p = 0.597) postoperatively in the endo-FODO and open FODO groups, respectively. Patients who underwent endo-FODO demonstrated significant improvements in margin-reflex distance 1 (MRD1) symmetry ratio (p = 0.004), palpebral height symmetry ratio (p = 0.004), canthal tilt symmetry (p = 0.020), and ODA (p = 0.009). Patients who underwent open FODO likewise demonstrated significant improvements in MRD1 symmetry ratio (p = 0.004), palpebral height symmetry ratio (p = 0.033), and ODA (p = 0.004). All postoperative measurements as well as degrees of improvement were similar between groups (p > 0.05).
Conclusions: Endo- and open FODO were associated with significant and comparable improvements in soft tissue periorbital symmetry and orbital dystopia at nearly two years postoperatively. While continued follow-up until cranial maturity is needed to assess the durability of aesthetic results, these data support a minimally invasive, endoscopic alternative to fronto-orbital distraction.
Keywords: Endoscopic; Fronto-orbital distraction osteogenesis; Minimally invasive; Unilateral coronal synostosis.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Competing interest: The authors declare no competing interests.
Figures


References
-
- Hoppe IC, Taylor JA (2021) A cohort study of strabismus rates following correction of the unicoronal craniosynostosis deformity: conventional bilateral fronto-orbital advancement versus fronto-orbital distraction osteogenesis. J Craniofac Surg 32(7):2362–2365. 10.1097/SCS.0000000000007773 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
