

2024 Update of the RECOVER-Adult Long COVID Research Index
- PMID: 39693079
- PMCID: PMC11862971
- DOI: 10.1001/jama.2024.24184
2024 Update of the RECOVER-Adult Long COVID Research Index
Abstract
Importance: Classification of persons with long COVID (LC) or post-COVID-19 condition must encompass the complexity and heterogeneity of the condition. Iterative refinement of the classification index for research is needed to incorporate newly available data as the field rapidly evolves.
Objective: To update the 2023 research index for adults with LC using additional participant data from the Researching COVID to Enhance Recovery (RECOVER-Adult) study and an expanded symptom list based on input from patient communities.
Design, setting, and participants: Prospective, observational cohort study including adults 18 years or older with or without known prior SARS-CoV-2 infection who were enrolled at 83 sites in the US and Puerto Rico. Included participants had at least 1 study visit taking place 4.5 months after first SARS-CoV-2 infection or later, and not within 30 days of a reinfection. The study visits took place between October 2021 and March 2024.
Exposure: SARS-CoV-2 infection.
Main outcomes and measures: Presence of LC and participant-reported symptoms.
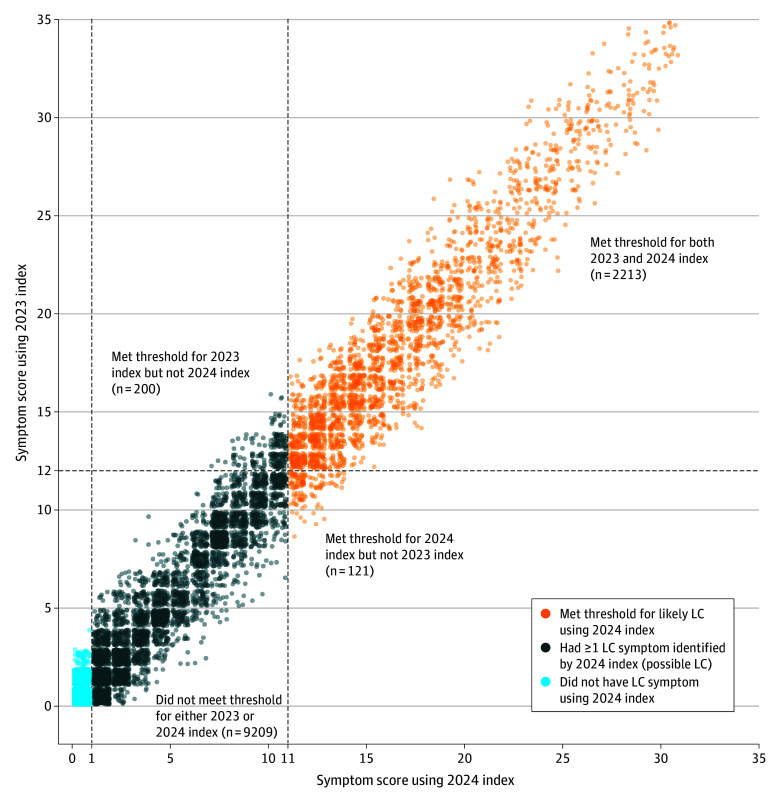
Results: A total of 13 647 participants (11 743 with known SARS-CoV-2 infection and 1904 without known prior SARS-CoV-2 infection; median age, 45 years [IQR, 34-69 years]; and 73% were female) were included. Using the least absolute shrinkage and selection operator analysis regression approach from the 2023 model, symptoms contributing to the updated 2024 index included postexertional malaise, fatigue, brain fog, dizziness, palpitations, change in smell or taste, thirst, chronic cough, chest pain, shortness of breath, and sleep apnea. For the 2024 LC research index, the optimal threshold to identify participants with highly symptomatic LC was a score of 11 or greater. The 2024 index classified 20% of participants with known prior SARS-CoV-2 infection and 4% of those without known prior SARS-CoV-2 infection as having likely LC (vs 21% and 5%, respectively, using the 2023 index) and 39% of participants with known prior SARS-CoV-2 infection as having possible LC, which is a new category for the 2024 model. Cluster analysis identified 5 LC subtypes that tracked quality-of-life measures.
Conclusions and relevance: The 2024 LC research index for adults builds on the 2023 index with additional data and symptoms to help researchers classify symptomatic LC and its symptom subtypes. Continued future refinement of the index will be needed as the understanding of LC evolves.
Conflict of interest statement
Figures

References
-
- US Centers for Disease Control and Prevention, National Center for Health Statistics . Long COVID: Household Pulse Survey. Accessed August 6, 2024. https://www.cdc.gov/nchs/covid19/pulse/long-covid.htm
-
- National Academies of Sciences, Engineering, and Medicine . A Long COVID Definition: A Chronic, Systemic Disease State With Profound Consequences. National Academies Press; 2024. - PubMed
Publication types
MeSH terms
Grants and funding
- OT2 HL156812/HL/NHLBI NIH HHS/United States
- R21 DC021054/DC/NIDCD NIH HHS/United States
- R01 HL151508/HL/NHLBI NIH HHS/United States
- R01 DC013277/DC/NIDCD NIH HHS/United States
- UM1 TR004528/TR/NCATS NIH HHS/United States
- OT2 HL161841/HL/NHLBI NIH HHS/United States
- R01 DC017397/DC/NIDCD NIH HHS/United States
- R01 HL162373/HL/NHLBI NIH HHS/United States
- UM1 TR004409/TR/NCATS NIH HHS/United States
- F31 DC006764/DC/NIDCD NIH HHS/United States
- OT2 HL161847/HL/NHLBI NIH HHS/United States
- R03 DC010267/DC/NIDCD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
