

Elevated concentrations of cardiac troponin T are associated with thoracic aortic calcification in non-dialysis chronic kidney disease patients of stage G3 to G5
- PMID: 39694530
- PMCID: PMC11656758
- DOI: 10.1080/0886022X.2024.2440512
Elevated concentrations of cardiac troponin T are associated with thoracic aortic calcification in non-dialysis chronic kidney disease patients of stage G3 to G5
Abstract
Background: Vascular calcification (VC), especially coronary artery calcification (CAC), serves as a robust predictor of cardiovascular mortality in chronic kidney disease (CKD) patients. Recent studies have revealed that the presence of extra-coronary calcifications (ECCs) contributes to cardiovascular disease (CVD). Elevated myocardial injury markers predict mortality risk in CKD patients and are associated with CVD. Nevertheless, the relationship between VC, including CAC and ECCs, and myocardial injury markers remain unexplored in non-dialysis CKD patients.
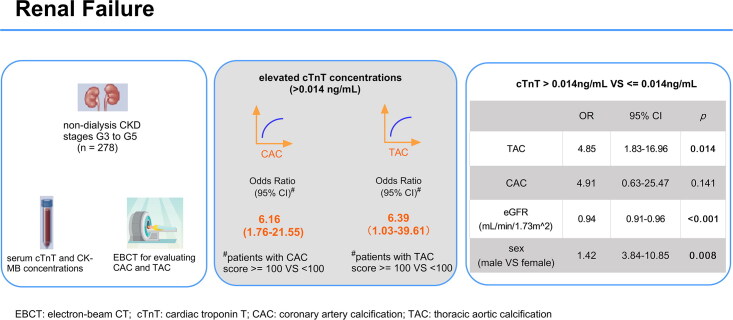
Methods: In 278 non-dialysis CKD patients of stage G3 to G5, we assessed calcified scores in CAC (Agatston score) and ECCs including thoracic aortic calcification (TAC), abdominal aortic calcification (AAC), carotid artery calcification, and valvular calcification. We analyzed the relationships between VC and myocardial injury markers of cardiac troponin T (cTnT) and creatine kinase-MB (CK-MB).
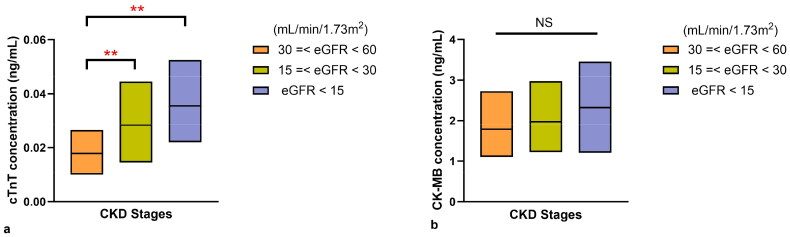
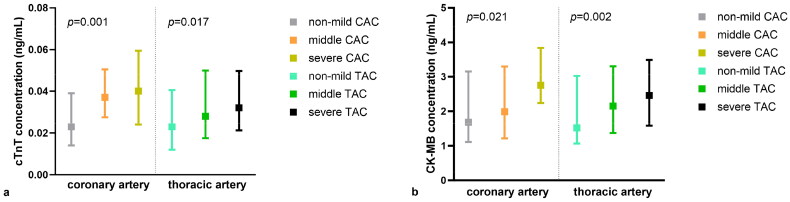
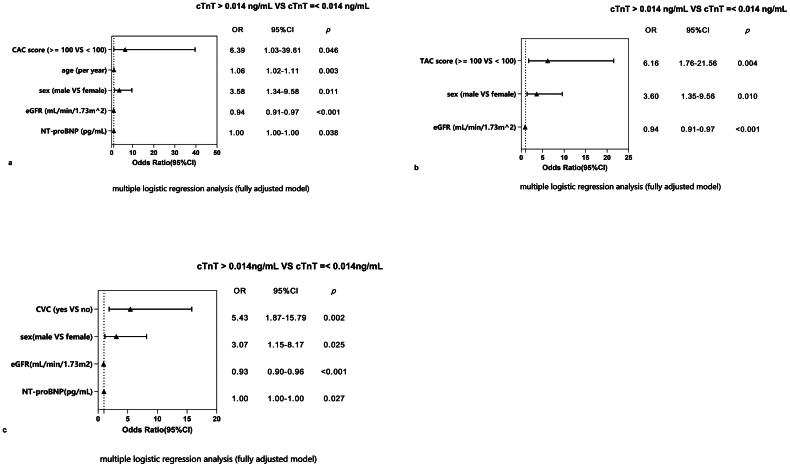
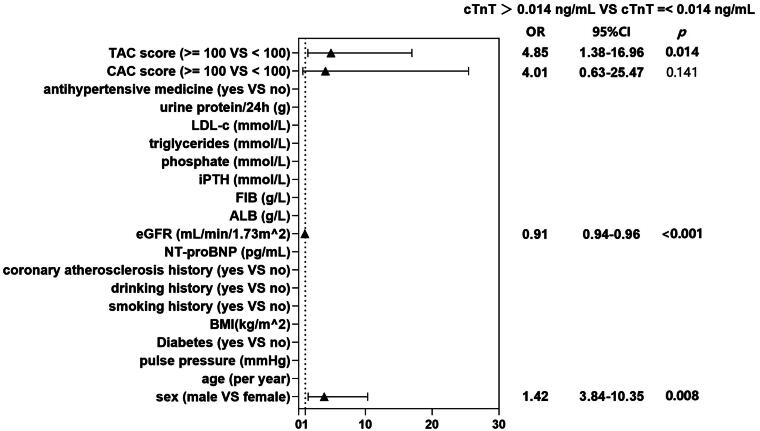
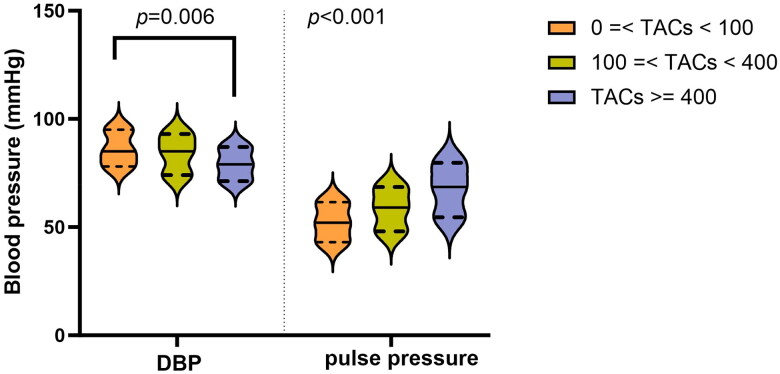
Results: A total of 278 non-dialysis CKD patients (median age 52.4 ± 13.2; male 65.1%; diabetes 33.5%) were enrolled. A total of 71.8% (227) of patients had cTnT levels above the upper limit of normal (> 0.014 ng/mL). Moderate to severe (calcified score ≥100 vs. <100), CAC (OR 6.39; 95% CI 1.03-39.61) and TAC (OR 6.16; 95% CI 1.76-21.55) were significantly associated with higher cTnT concentrations after adjustment for confounders. Additionally, male sex and a lower eGFR were also associated with cTnT elevation. However, when we included CAC and TAC in one model, only moderate to severe TAC (OR 4.85; 95% CI 1.38-16.96) was a risk factor for cTnT elevation, but not CAC. Furthermore, patients with severer TAC presented lower diastolic blood pressure (DBP), wider pulse pressure (p < 0.001) and higher prevalence of left ventricular hypertrophy (LVH).
Conclusion: Moderate to severe thoracic aortic calcification (TAC score ≥ 100) is significantly associated with elevated cTnT concentrations in non-dialysis CKD patients of stage G3 to G5. The linkage may result from decreased coronary perfusion and relative myocardial ischemia.
Keywords: Coronary artery calcification; cardiac troponin T; chronic kidney disease; creatine kinase-MB; thoracic aortic calcification.
Plain language summary
Vascular calcification (VC), including coronary artery calcification (CAC) and extra-coronary calcifications (ECCs), is recognized as a strong predictor of cardiovascular mortality in patients with chronic kidney disease (CKD). In this study involving 278 non-dialysis CKD patients of stage G3 to G5, we assessed the calcification scores for CAC, thoracic aortic calcification (TAC), abdominal aortic calcification (AAC), carotid artery calcification, and valvular calcification. And explored relationship between VC and myocardial injury markers such as cardiac troponin T (cTnT) and creatine kinase-MB (CK-MB). The study found that cTnT levels were associated with the severity of CAC (OR 6.39; 95% CI 1.03-39.61) and TAC (OR 6.16; 95% CI 1.76-21.55). After adjusting for confounding factors, only moderate to severe TAC (OR 4.85; 95% CI 1.38-16.96) was identified as a significant risk factor for elevated cTnT levels, but not CAC. Furthermore, the potential association between TAC and myocardial ischemia may be due to decreased coronary perfusion and left ventricular hypertrophy (LVH). These findings underscore the importance of monitoring TAC which may be more effectively associated with cardiovascular risks.
Conflict of interest statement
The authors report there are no competing interests to declare.
Figures
References
-
- Shroff GR, Sanchez OA, Miedema MD, et al. . Coronary artery calcium progresses rapidly and discriminates incident cardiovascular events in chronic kidney disease regardless of diabetes: the Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis. 2020;310:75–82. doi: 10.1016/j.atherosclerosis.2020.07.026. - DOI - PMC - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous