

Personalized neoantigen hydrogel vaccine combined with PD-1 and CTLA-4 double blockade elicits antitumor response in liver metastases by activating intratumoral CD8+CD69+ T cells
- PMID: 39694701
- PMCID: PMC11660327
- DOI: 10.1136/jitc-2024-009543
Personalized neoantigen hydrogel vaccine combined with PD-1 and CTLA-4 double blockade elicits antitumor response in liver metastases by activating intratumoral CD8+CD69+ T cells
Abstract
Background: Liver metastasis is highly aggressive and immune tolerant, and lacks effective treatment strategies. This study aimed to develop a neoantigen hydrogel vaccine (NPT-gels) with high clinical feasibility and further investigate its efficacy and antitumor molecular mechanisms in combination with immune checkpoint inhibitors (ICIs) for the treatment of liver metastases.
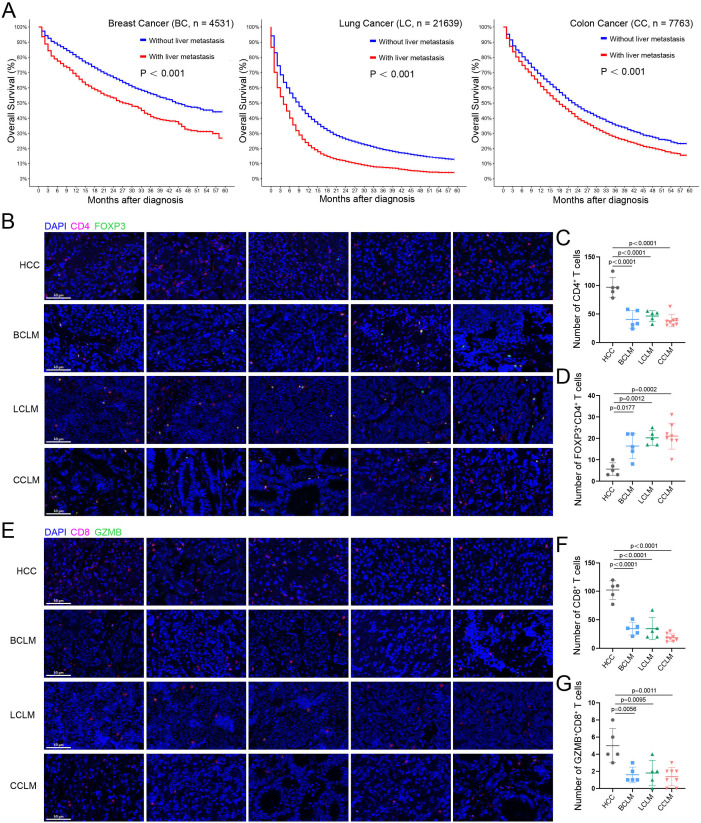
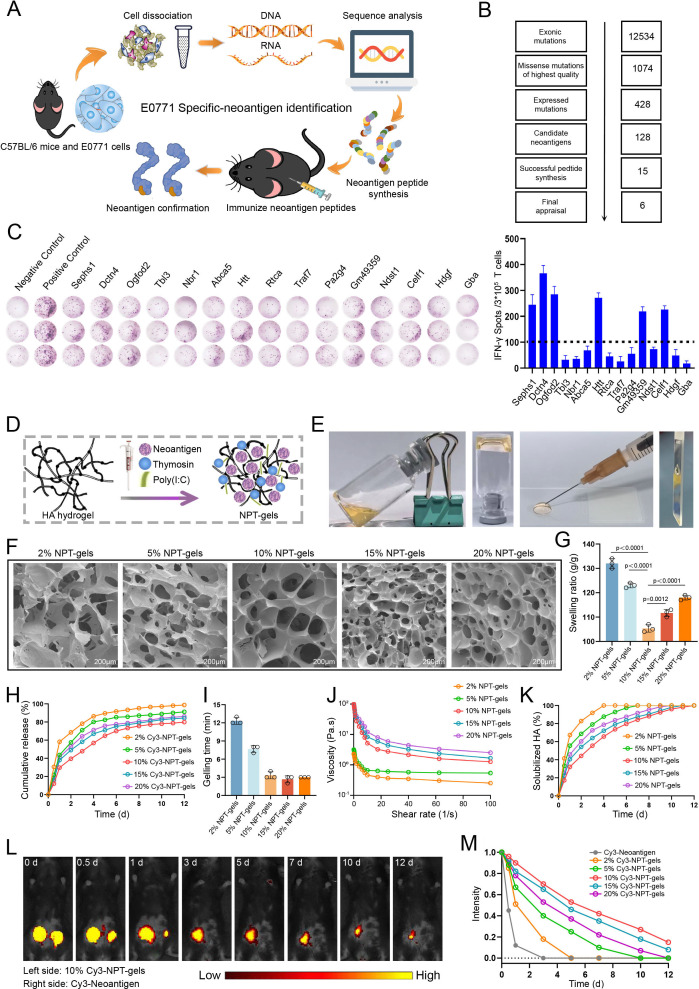
Methods: The effects of liver metastasis on survival and intratumor T-cell subpopulation infiltration in patients with advanced tumors were investigated using the Surveillance, Epidemiology, and End Results Program (SEER) database and immunofluorescence staining, respectively. NPT-gels were prepared using hyaluronic acid, screened neoantigen peptides, and dual clinical adjuvants [Poly(I:C) and thymosin α-1]. Then, the efficacy and corresponding antitumor molecular mechanisms of NPT-gels combined with programmed death receptor 1 and cytotoxic T-lymphocyte-associated protein 4 double blockade (PCDB) for the treatment of liver metastases were investigated using various preclinical liver metastasis models.
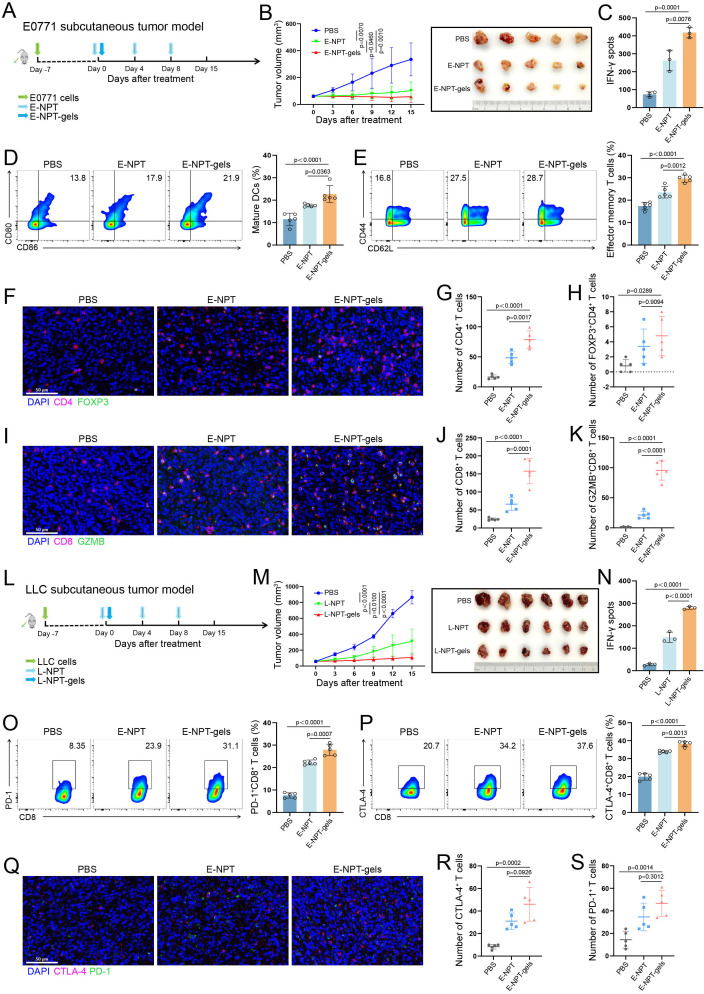
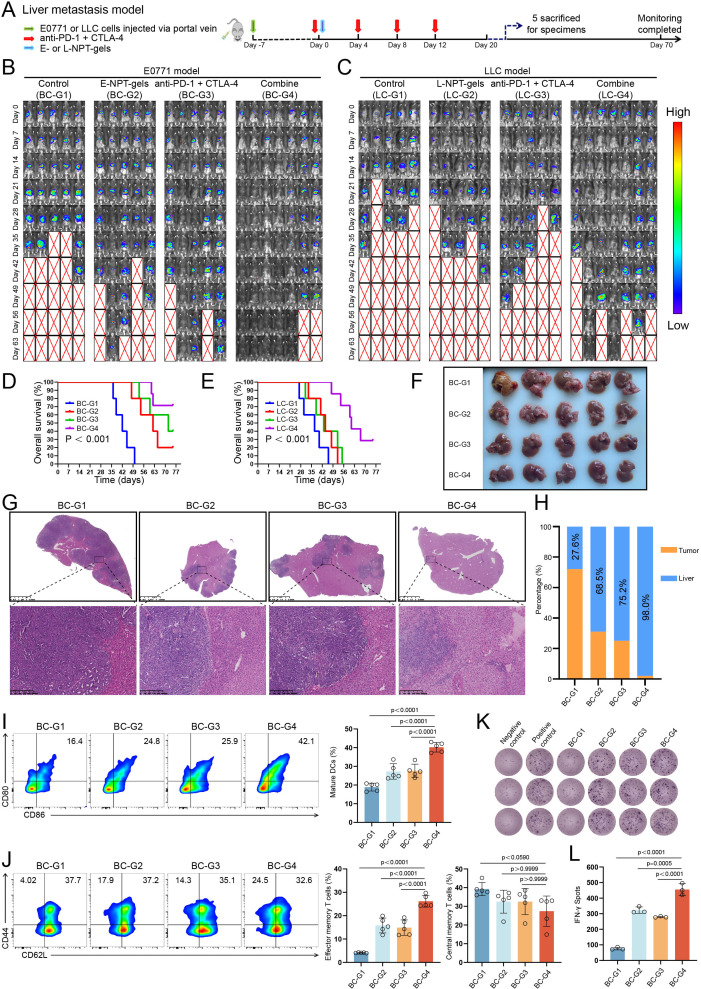
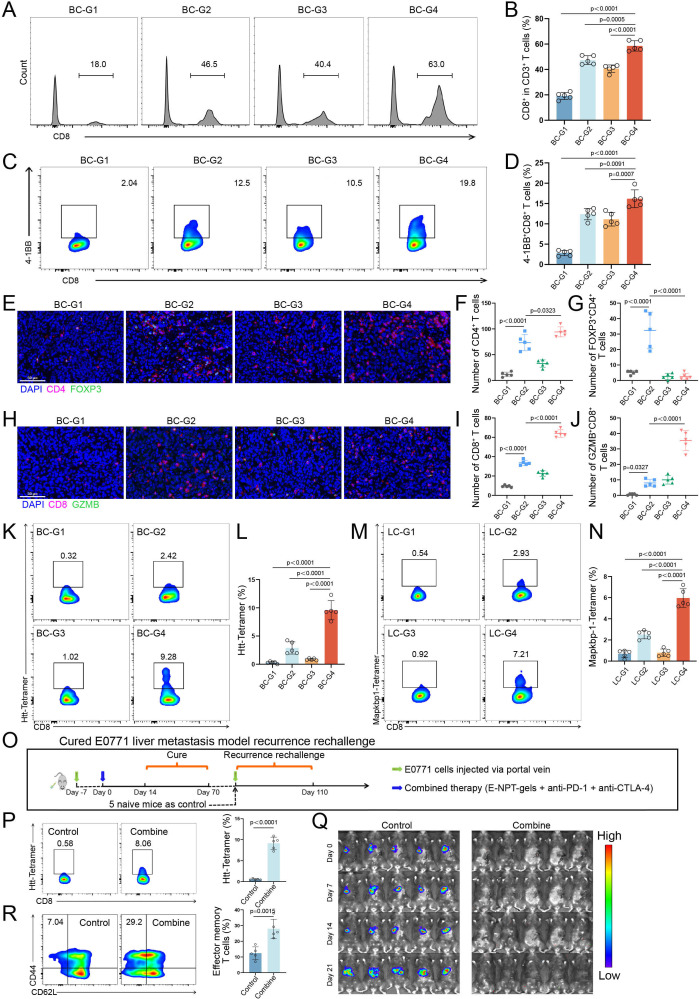
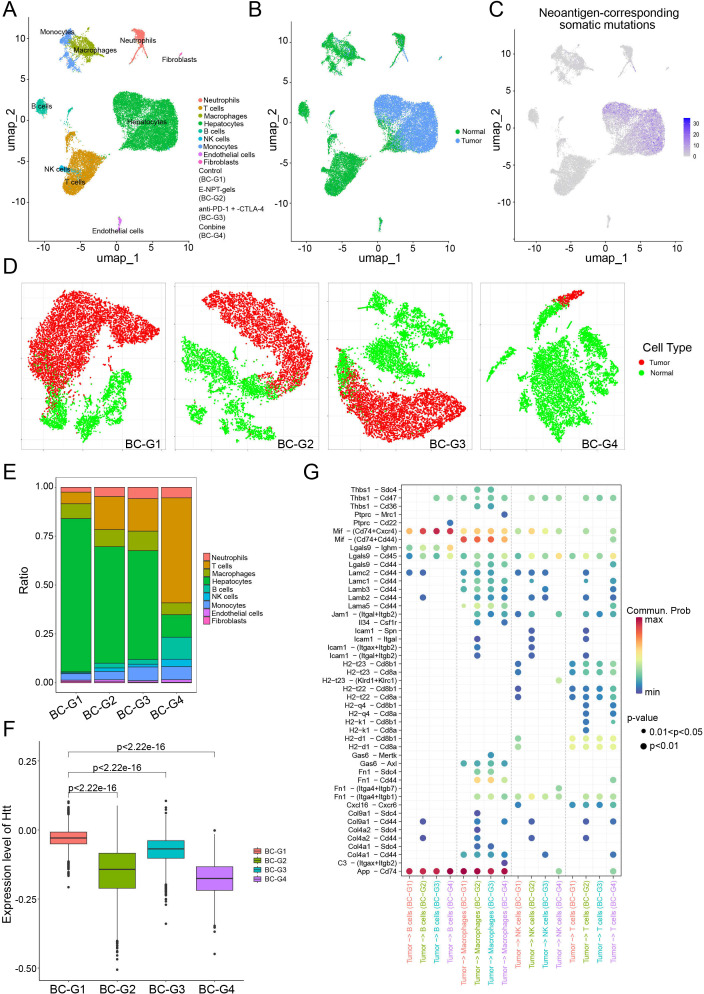
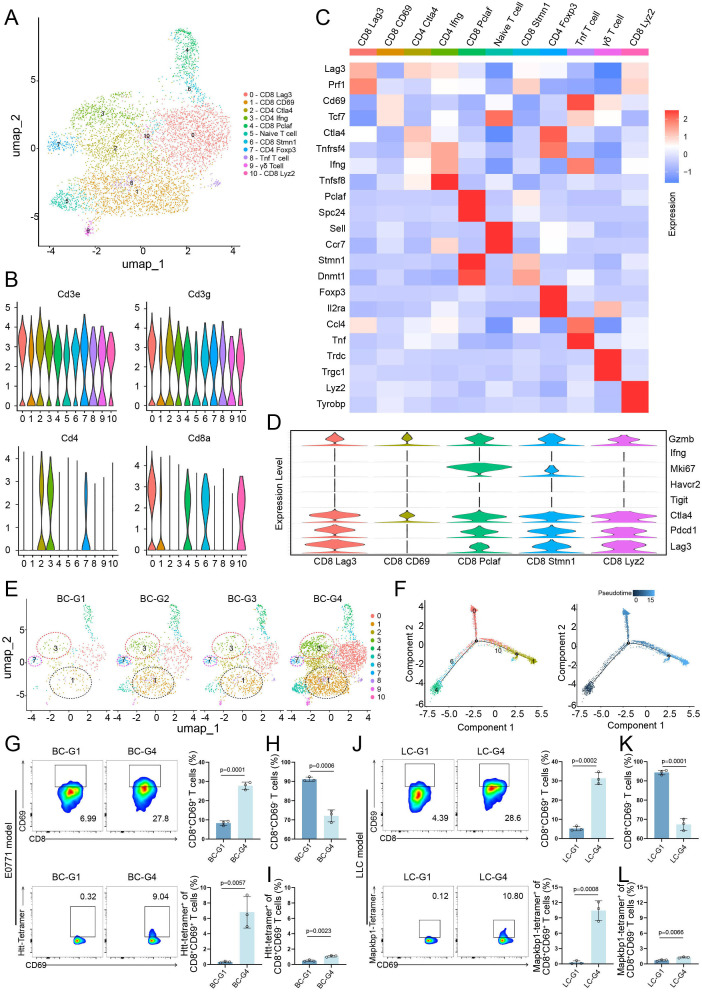
Results: Liver metastases are associated with poorer 5-year overall survival, characterized by low infiltration of cytotoxic CD8+ T cells and high infiltration of regulatory T cells (Tregs). NPT-gels overcame the challenges faced by conventional neoantigen peptide vaccines by sustaining a durable, high-intensity immune response with a single injection and significantly improving the infiltration of neoantigen-specific T-cell subpopulations in different mice subcutaneous tumor models. Importantly, NPT-gels further combined with PCDB could enhance neoantigen-specific T-cell infiltration and effectively unlock the immunosuppressive microenvironment of liver metastases, showing superior antitumor efficacy and inducing long-term immune memory in various preclinical liver metastasis models without obvious toxicity. Mechanistically, the combined strategy can inhibit Tregs, induce the production and infiltration of neoantigen-specific CD8+CD69+ T cells to enhance the immune response, and potentially elicit antigen-presenting effects in Naïve B_Ighd+ cells and M1-type macrophages.
Conclusions: This study demonstrated that NPT-gels combined with PCDB could exert a durable and powerful antitumor immunity by enhancing the recruitment and activation of CD8+CD69+ T cells, which supports the rationale and clinical translation of this combination strategy and provides important evidence for further improving the immunotherapy efficacy of liver metastases in the future.
Keywords: T cell; T regulatory cell - Treg; immune checkpoint inhibitor; immunotherapy; vaccine.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: No, there are no competing interests.
Figures
Similar articles
-
Personalized neoantigen vaccine combined with PD-1 blockade increases CD8+ tissue-resident memory T-cell infiltration in preclinical hepatocellular carcinoma models.J Immunother Cancer. 2022 Sep;10(9):e004389. doi: 10.1136/jitc-2021-004389. J Immunother Cancer. 2022. PMID: 36113894 Free PMC article.
-
Comparing neoantigen cancer vaccines and immune checkpoint therapy unveils an effective vaccine and anti-TREM2 macrophage-targeting dual therapy.Cell Rep. 2024 Nov 26;43(11):114875. doi: 10.1016/j.celrep.2024.114875. Epub 2024 Oct 23. Cell Rep. 2024. PMID: 39446585 Free PMC article.
-
Immune checkpoint Ab enhances the antigen-specific anti-tumor effects by modulating both dendritic cells and regulatory T lymphocytes.Cancer Lett. 2019 Mar 1;444:20-34. doi: 10.1016/j.canlet.2018.11.039. Epub 2018 Dec 10. Cancer Lett. 2019. PMID: 30543813
-
CTLA-4 and PD-1 combined blockade therapy for malignant melanoma brain metastases: mechanisms, challenges, and prospects.Front Immunol. 2025 Jul 1;16:1629879. doi: 10.3389/fimmu.2025.1629879. eCollection 2025. Front Immunol. 2025. PMID: 40666508 Free PMC article. Review.
-
Treg-mediated acquired resistance to immune checkpoint inhibitors.Cancer Lett. 2019 Aug 10;457:168-179. doi: 10.1016/j.canlet.2019.05.003. Epub 2019 May 9. Cancer Lett. 2019. PMID: 31078738 Review.
Cited by
-
Targeting Mesothelin Enhances Personalized Neoantigen Vaccine Induced Antitumor Immune Response in Orthotopic Pancreatic Cancer Mouse Models.Adv Sci (Weinh). 2025 Mar;12(12):e2407976. doi: 10.1002/advs.202407976. Epub 2025 Jan 31. Adv Sci (Weinh). 2025. PMID: 39887656 Free PMC article.
-
Deep learning radiomics based on MRI for differentiating tongue cancer T - staging.BMC Cancer. 2025 Aug 22;25(1):1358. doi: 10.1186/s12885-025-14627-6. BMC Cancer. 2025. PMID: 40847271 Free PMC article.
-
Application of Immune Checkpoint Inhibitors in Cancer.MedComm (2020). 2025 Aug 10;6(8):e70176. doi: 10.1002/mco2.70176. eCollection 2025 Aug. MedComm (2020). 2025. PMID: 40787068 Free PMC article. Review.
-
Multifaceted functions of tissue-resident memory T cells in tumorigenesis and cancer immunotherapy.Cancer Immunol Immunother. 2025 Apr 26;74(6):184. doi: 10.1007/s00262-025-04035-x. Cancer Immunol Immunother. 2025. PMID: 40285796 Free PMC article. Review.
-
Targeting Antigen-Presenting Cells to Enhance the Tumor-Spleen Immunity Cycle through Liposome-Neoantigen Vaccine.Adv Sci (Weinh). 2025 May;12(19):e2500021. doi: 10.1002/advs.202500021. Epub 2025 Mar 24. Adv Sci (Weinh). 2025. PMID: 40125791 Free PMC article.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials