

Optimizing prone CT use for suspected interstitial lung abnormalities
- PMID: 39694885
- PMCID: PMC12081487
- DOI: 10.1007/s00330-024-11259-5
Optimizing prone CT use for suspected interstitial lung abnormalities
Abstract
Objectives: We investigated whether supine chest CT alone suffices for diagnosing ILAs, thereby reducing the need for prone chest CT.
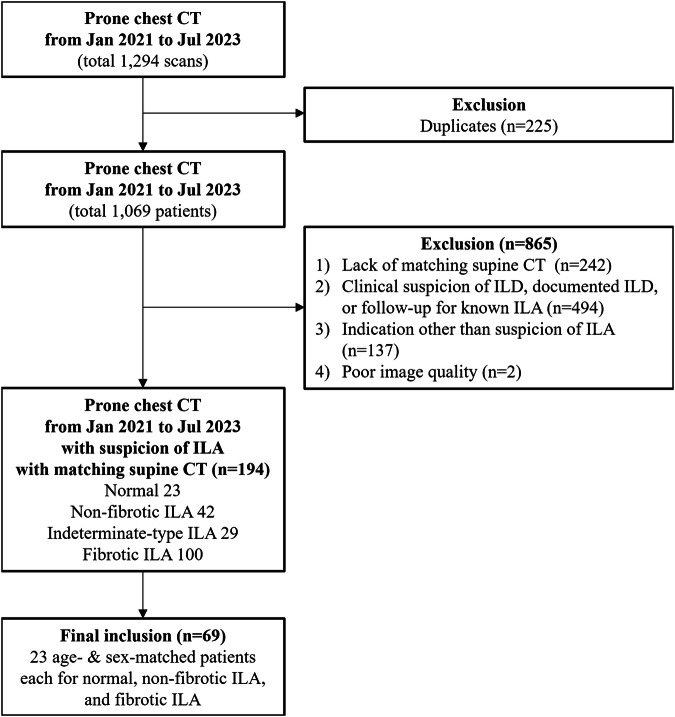
Materials and methods: Patients who underwent prone chest CT for suspected ILAs from January 2021 to July 2023, with matching supine CT within 1 year, were retrospectively evaluated. Five multinational thoracic radiologists independently rated ILA suspicion and fibrosis scores (1 to 5-point) and ILA extent (1-100%) using supine CT first, then combined supine-prone CT after a 1-month washout. We categorized ILA suspicion and fibrosis scores into four diagnostic groups; normal, non-fibrotic, indeterminate-type, and fibrotic ILAs. The areas under the receiver operating characteristic curve (AUCs) of ILA suspicion scores, inter-reader agreement on diagnostic categories, and intra-reader/inter-reader reliability for ILA extent were evaluated.
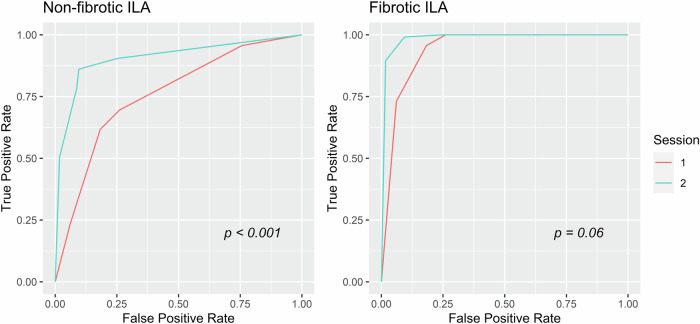
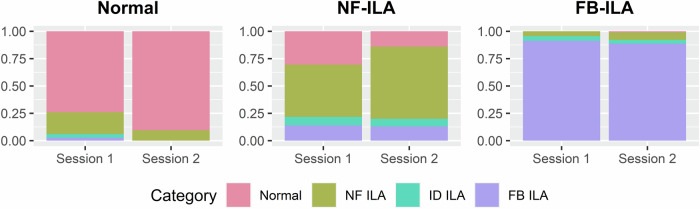
Results: This study included 69 patients (mean age 67.2 ± 7.2 years; 36 women), with 23 age- and sex-matched patients in each group: normal, non-fibrotic ILAs, and fibrotic ILAs. The pooled AUC for ILA suspicion and inter-reader agreement on diagnostic categories improved for non-fibrotic ILAs with prone CT (AUC 0.76 to 0.92, p < 0.001; Fleiss kappa 0.25 to 0.51, p = 0.004), but not for fibrotic ILAs (AUC 0.94 to 0.99, p = 0.06; Fleiss kappa 0.63 to 0.72, p = 0.08). ILA extent was 1-2% smaller with prone CT for both ILA types (p < 0.001).
Conclusion: For fibrotic ILAs, supine CT alone exhibited substantial diagnostic accuracy and inter-reader agreement, while the diagnosis of non-fibrotic ILAs benefited from adding prone CT. Supine CT alone slightly overestimated extent regardless of ILA type.
Key points: Question Prone CT is recommended when interstitial lung abnormalities (ILAs) are suspected on supine CT, but its benefits remain underexplored. Findings Supine CT alone sufficed for diagnosing fibrotic ILAs, while prone CT improved non-fibrotic ILA diagnosis and reduced extent overestimation for both types. Clinical relevance Omitting prone CT reduces extra time, space, and radiation exposure without compromising the diagnosis of fibrotic ILAs, which have higher rates of progression and mortality risks, enhancing patient comfort and simplifying patient management.
Keywords: Interstitial lung abnormality; Lung diseases (Interstitial); Prone CT; Pulmonary atelectasis; Tomography (X-ray computed).
© 2024. The Author(s).
Conflict of interest statement
Compliance with ethical standards. Guarantor: The scientific guarantor of this publication is S.H.Y. Conflict of interest: M.Y. is a member of the Scientific Editorial Board for European Radiology (section: chest). S.H.Y. holds stocks and stock options of MEDICAL IP, unrelated to this work. The remaining authors of this manuscript declare no relationships with any companies, whose products or services may be related to the subject matter of the article. Statistics and biometry: One of the authors, M.J.J., has significant statistical expertise. Informed consent: Written informed consent was waived by the Institutional Review Board. Ethical approval: Institutional Review Board approval was obtained. Study subjects or cohorts overlap: None of the study subjects or cohorts have been previously reported. Methodology: Retrospective Diagnostic or prognostic study Performed at one institution
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
