

The impact of a fracture liaison service with in-hospital anti-osteoporosis treatment on subsequent hip fracture and mortality rates-a single-center retrospective study
- PMID: 39694923
- PMCID: PMC11825567
- DOI: 10.1007/s00198-024-07325-9
The impact of a fracture liaison service with in-hospital anti-osteoporosis treatment on subsequent hip fracture and mortality rates-a single-center retrospective study
Abstract
The implementation of an in-hospital fracture liaison service facilitated prompt initiation of anti-osteoporosis treatment following a hip fracture (HF), increasing follow-up and treatment rates. This led to a 48% reduction in the risk of subsequent HF and a 29% decrease in mortality rates.
Purpose: To demonstrate the impact of an institutional fracture liaison service (FLS) which allowed in-hospital anti-osteoporosis treatment following hip fracture (HF) on subsequent HF and mortality rate.
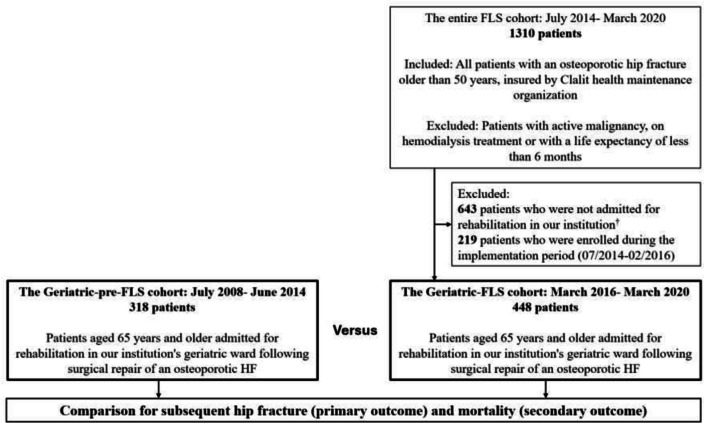
Methods: We retrospectively evaluated patients aged 65 years and older, admitted with an osteoporotic HF, who were transferred following surgery for rehabilitation in the geriatrics department in two time periods: before and after the implementation of an institutional FLS ("geriatric-pre-FLS" and "geriatric-FLS" cohorts, respectively). Data were captured from electronic records and the two cohorts were compared following an assessment of baseline characteristics, follow-up, and anti-osteoporosis treatment initiation. A multivariable Cox regression model evaluated differences between the cohorts regarding subsequent HF and mortality rates.
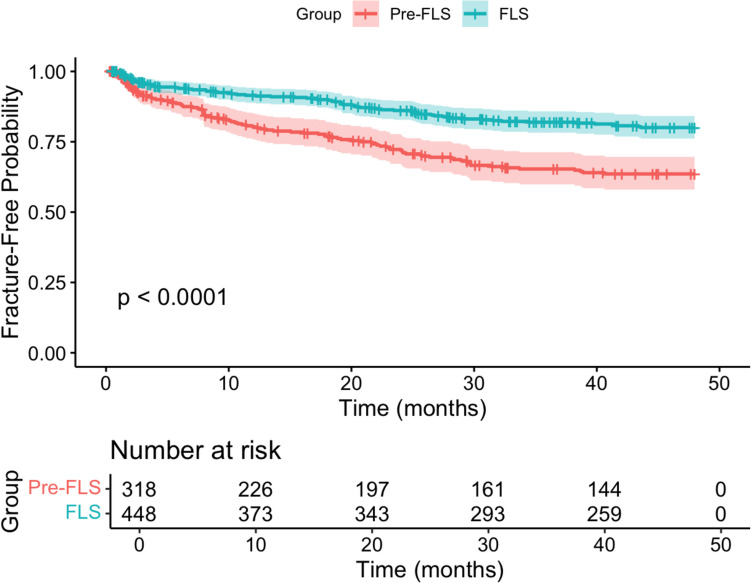
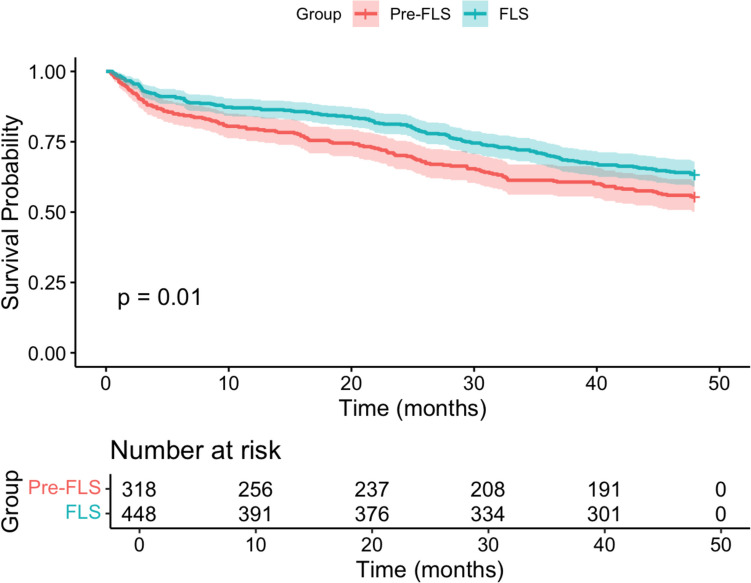
Results: Three hundred and eighteen and 448 patients comprised the geriatric-pre-FLS (07/2008-06/2014) and the geriatric-FLS (03/2016-03/2020) cohorts, respectively. Baseline characteristics were comparable between the cohorts (median age 81 vs. 82, p = 0.08 and female sex 73% vs. 70%, p = 0.48, respectively). Rates of endocrine consultation (3.5% vs. 99%%, p < 0.001), DXA-BMD testing (7.5% vs. 34%, p < 0.001), and parenteral anti-osteoporosis treatment (4% vs. 76.6%, p < 0.001) were all higher in the geriatric-FLS cohort. The implementation of the FLS led to a 48% reduction in subsequent HF risk (HR 0.52; 95% CI 0.37-0.74, p < 0.001) and a 29% decrease in mortality rate (HR 0.71; 95% CI 0.54-0.92, p = 0.011).
Conclusions: The implementation of an in-hospital FLS facilitated prompt initiation of anti-osteoporosis treatment following a HF, increased follow-up and treatment rates, and resulted in a 48% reduction in subsequent HF risk and a 29% reduction in mortality rates.
Keywords: Fracture liaison services (FLS); Hip fracture; Mortality; Osteoporosis; Subsequent hip fracture.
© 2024. The Author(s).
Conflict of interest statement
Declarations. Ethical approval: All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent: For this type of study, formal consent is not required. Conflicts of interest: None.
Figures
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
