

Clinico-pathological predictors of radiologic complete response to first-line anti-HER2 therapy in metastatic breast cancer
- PMID: 39695115
- PMCID: PMC11655875
- DOI: 10.1038/s41523-024-00713-8
Clinico-pathological predictors of radiologic complete response to first-line anti-HER2 therapy in metastatic breast cancer
Abstract
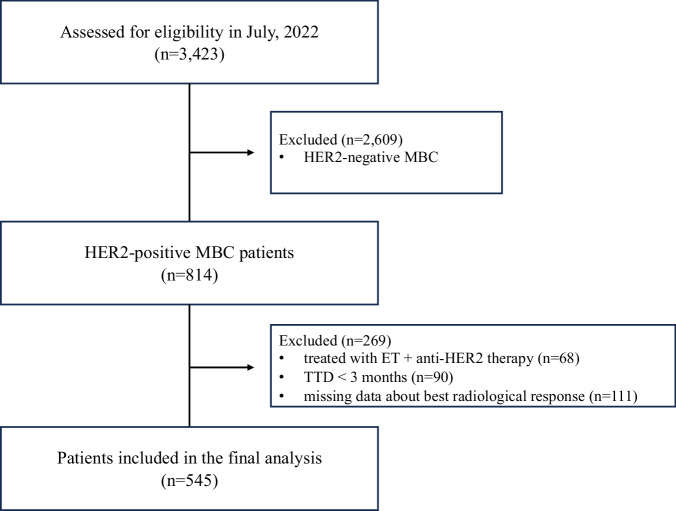
This study aimed to identify the clinico-pathological variables predictive of radiologic complete response (rCR) to first-line anti-HER2 therapy in patients with HER2-positive metastatic breast cancer. Patients were selected from the database of the GIM14 study and classified according to the best radiologic response obtained to first-line anti-HER2 therapy and upon time-to-treatment-discontinuation (TTD). A total of 545 patients were included in the analysis. Eighty patients experienced a rCR to first-line anti-HER2 therapy with a TTD > 3 months and HER2 Immunohistochemistry score 3+, presence of non-visceral metastases and 1 metastatic site were significantly associated with higher odds of obtaining a CR. Of the 80 patients achieving a rCR, 56 experienced a CR with a TTD > 18 months, with anti-HER2 therapy being the only variable significantly associated with a higher probability of achieving such sustained CR.
© 2024. The Author(s).
Conflict of interest statement
Competing interests: E.B.: grants from Gilead to institution; personal fees from Eli Lilly; C.B.: fees or honoraria from Novartis, Roche and Eli Lilly; A.F.: advisory boards: Roche, Novartis, Eli Lilly, Pfizer, MSD, Pierre Fabre, Eisai, Gilead, Seagen, AstraZeneca, Exact Sciences; consulting fees: Dompé Farmaceutici S.p.A.; F.M.: consulting fees: Roche, Novartis, AstraZeneca, Daiichy Sankyo, SeaGen, MSD, Eli Lilly, Pfizer, and Pierre Fabre; travel grants: Roche and AstraZeneca; from May 15th, 2023, F.M. is Roche employee (all the disclosed activities are outside the submitted work); M.D.L.: speaker’s honoraria, consulting honoraria, and advisory board honoraria: Novartis, Eli Lilly, Pfizer, Roche, Sophos, Genetic, Menarini, Daiichi-Sankyo, Seagen, Pierre Fabre, GSK and Takeda; G.A.: research and medical writing: AstraZeneca; advisory boards, travel grants, activities as a speaker, consultancy: AstraZeneca, Daiichi Sankyo, Eisai, Eli Lilly, Gilead, Exact Science, Novartis, Roche, Seagen, Viatris; L.D.M.: institutional grants: Eli Lilly, Novartis, Roche, Daiichi Sankyo, Seagen, Astra Zeneca, Gilead, Pierre Fabre; consulting fees: Eli Lilly, Gilead, Daiichi Sankyo; payment or honoraria for lectures, presentations, speakers bureaus: Roche, Novartis, Pfizer, Eli Lilly, AstraZeneca, MSD, Seagen, Gilead, Pierre Fabre, Eisai, Exact Sciences, Ipsen, GSK, Agendia, Menarini Stemline; support for attending meetings and/or travel: Roche, Pfizer, Eisai, Daiichi Sankyo, AstraZeneca, Gilead; Participation on a Data Safety Monitoring Board or Advisory Board: Novartis, Roche, Eli Lilly, Pfizer, Daiichi Sakyo, Exact Sciences, Gilead, Pierre Fabre, Eisai, AstraZeneca, Agendia, GSK, Seagen, Olema, MSD, Menarini Stemline; L.G.: consulting or advisory role: AstraZeneca, Daiichi Sankyo, Eli Lilly, GlaxoSmithKline, Incyte, Novartis, Pfizer, Merck Sharp & Dohme, Menarini Stemline, Abbvie; research funding: Menarini Silicon Biosystems Patents, Royalties; travel expenses: Menarini Stemline; F.P.: honoraria for advisory boards, activities as a speaker, travel grants, research grants from Amgen, AstraZeneca, Daiichi Sankyo, Celgene, Eisai, Eli Lilly, Exact Sciences, Gilead, Ipsen, Menarini, MSD, Novartis, Pierre Fabre, Pfizer, Roche, Seagen, Takeda, Viatris; research funding from AstraZeneca, Eisai, Roche, outside the submitted work. The remaining authors have no conflict to disclose.
Figures



References
-
- Sung, H. et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin.71, 209–249 (2021). - PubMed
-
- Slamon, D. J. et al. Use of chemotherapy plus a monoclonal antibody against HER2 for metastatic breast cancer that overexpresses HER2. N. Engl. J. Med.344, 783–792 (2001). - PubMed
-
- Yeo, B., Kotsori, K., Mohammed, K., Walsh, G. & Smith, I. E. Long-term outcome of HER2 positive metastatic breast cancer patients treated with first-line trastuzumab. Breast24, 751–757 (2015). - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
